This understatement is a useful rule of thumb for grasping the carnage inflicted by the genetic vaccines. It is well documented in the medical literature that covid in rare cases can cause damage to almost any part of the human anatomy, even the harder-to-reach, protected areas (“privileged tissues”). The vaccines however unleash a massive tsunami of LNP’s and spike proteins that can end up anywhere - or everywhere - precipitating widespread carnage wherever vaccine product lands.
Which brings us to today’s topic: Reproductive tissues of the male anatomy. Or more specifically, a rare, sometimes painful, but always embarrassing condition that is likely to have one of the most extreme underreporting factors (URF) of any vaccine injury type.
When it comes to reproductive adverse events from the covid vaccines, the focus has pretty much centered around female reproductive issues, leaving the male side a bit under-discussed, which we shall try to remedy at least a little.
In my journey through the bottomless well of vaccine injury case reports (about 2,200 compiled so far), I came across the following two reports covering 6 cases of Penile Mondor Disease or PMD (essentially clotting in the penile vasculature), that I suspect might be the tip of a rather large iceberg of SAE’s:
First, what is PMD? Here’s how the authors of study #2 describe it:
Usually, PMD is an under-reported benign, self-limited disease that resolves spontaneously in four to eight weeks. The PMD under reporting may be because the lesion is often non painful and self-resolving. Most patients refrain from seeking medical attention, and when they do, sometimes even physicians pay little attention to the lesion. The PMD pathogenesis can be demonstrated by Virchow’s triad.
PMD can cause significant patient anxiety and embarrassment and may be easily confused with more concerning conditions.
Covid can in rare instances lead to PMD, which the authors of both studies point out, including the following two citations from study #112. This is plausible, because covid especially at the beginning was this crazy clot machine. Just ask any ICU doc who was working in NYC during March 2020.
The fact that this is a documented sequelae of covid infection suggests that it is likewise plausible - expected even - for PMD to similarly manifest as a post-vaccine sequelae, because the vaccines and covid share the primary biological antagonist that leads to many of the known adverse pathologies of covid, especially the blood clotting: the highly toxic spike protein.
Continuing with their report:
Nothing is reported in the literature regarding the possible relationship between vaccination against Covid-19 and PMD. However, in our daily clinical practice, in the last three months, we have recorded an increase in outpatient assessments of PMD.
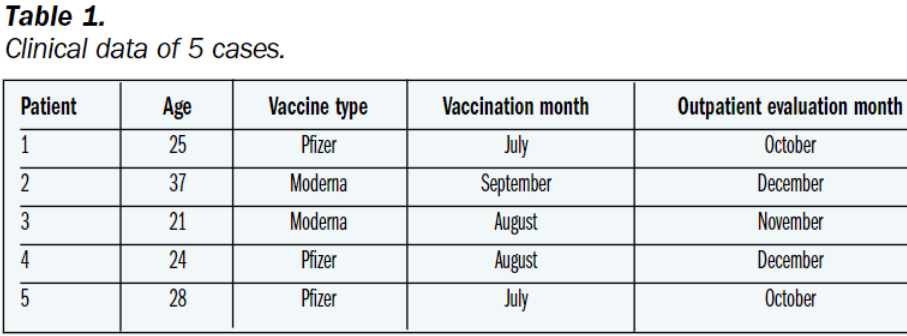
We refer to 5 cases whose clinical data are reported in Table 1:
Clinical course of disease:
Only the symptomatic patients (2/5) were treated with analgesic. Only one case (1/5) received low molecular weight heparin for 15 days. All patient reported complete recovery from symptoms and subcutaneous cord-like indurations complained at the presentation.
Here’s the kicker (emphasis added):
No patients declared prolonged or unusual sexual activity. The clinical histories were silent for any possible hypercoagulability status. Vaccinations were the only possible pathogenetic factors linking the 5 young patients.
Yup, the vaccines are the overwhelming odds-on bet as the cause of these cases of PMD.
Let’s turn to the other study. Their clinical narrative description speaks for itself:
This case report describes the first published case of penile thrombophlebitis after administration of the AstraZeneca ChAdOx1-S vaccine, a now well-documented precipitant of a heightened prothrombotic state that is highly relevant during the current ongoing pandemic3.
A 59-year-old man presented to his general practitioner due to 7 days of pain and inflammation of the proximal one-third of his penis. He recounted no recent genitourinary infections, trauma or previous concerns about his penis. As regards his medical history, he had previously been noted to have mild hypertension and was not on any regular medications. Examination revealed inflammation at the base of the penis, and a firm palpable rope-like vein on the left dorsum. A urine dipstick was negative for infection, and he did not undergo a panel of blood tests at this stage. It was noted that 7 days prior to his symptoms he had been administered his first dose of the AstraZeneca ChAdOx1-S vaccine.
Due to the symptomatology, he underwent colour Doppler ultrasound of the penis, which revealed an echogenic tubular structure measuring 2 mm at the base of the penis extending along the painful line, consistent with PMD.
One week later, he had taken paracetamol and ibuprofen for pain and his symptoms had nearly resolved.
Due to symptom resolution, no further treatment was deemed necessary.
The authors conclude:
The authors suggest this case demonstrates a rare sequela of AstraZeneca ChAdOx1-S vaccination not yet reported in the literature. While it is unfortunate an initial blood panel was not taken to detect coagulation abnormalities to support this diagnosis, the absence of any other discussed risk factor beyond the recent vaccination in the patient leads us to believe it was the precipitating event. This case corroborates incoming data suggesting ChAdOx1-S vaccination places patients at low but appreciable increased risk of venous thrombotic events. While widespread vaccination is and should be endorsed to control the significant health and economic costs of COVID-19, it is a reminder that clinicians must be wary of a wide variety of side effects, particularly thrombosis in the otherwise well patient.
So all in all, 3/6 cases were symptomatic enough to require medical intervention, and all six are described as having fully recovered.
Takeaways
A few things stood out to me:
PMD is probably one of the most proportionately underreported vaccine adverse events. Men are strongly dispositioned psychologically to avoid revealing a condition such as PMD that involves male genitalia. This would be especially true regarding adolescents.
It took an average of a few months from vaccination to manifestation of clinical symptoms.
While everyone from both studies recovered and PMD is generally “self-limiting”, it is impossible to draw firm conclusions from a sample size of 6 patients. It is also possible that the recovery is incomplete, as there may be a lingering ongoing subclinical pathology.
We don’t know what the specific pathology leading to these penile thrombotic events is. For all we know, there may be lingering damage to the penile vasculature that can manifest later. It is entirely reasonable that this pathology might eventually result in permanent ED in some men.
Any vaccine adverse event is an indication that the vaccine is causing harm generally. Dr. Flavio Cadegianni related a few months ago in one of the FLCCC weekly zoom events that every single patient he saw who had a vaccine injury, regardless of the nature of the injury, also showed subclinical myocarditis on cardiac MRI. In other words, when the vaccine is inflicting injury, there is no basis to assume that it is limited to the manifesting clinical symptoms a patient presents with.
I will leave it to the reader to derive a conclusion from these observations.
Another critical observation here is something (surprisingly) bluntly articulated by the authors of the 5-case series: (emphasis added)
The questions arising from this real-life experience are basically two. Is it therefore possible that there is a pathogenetic link between PMD and vaccination anti Covid-19? Is there any possibility of identifying subjects predisposed to the onset of this vascular disease after vaccination? Although the PMD clinical course is very often self-limiting, in a scenario characterized by an annual anti-Covid vaccination, may be important to always inform young male about the eventuality of developing PMD and alert general practitioners and referral specialists about the possible increase in the PMD response.
Yeah, it may be prudent to know what the effects of repeated dosing are before embarking on a reckless and aggressive endless series of booster shots. I doubt that there will be any missives going out to GP’s though.
PMD comes after other potentially embarrassing injuries to male reproductive anatomy. Nikki Minaj tweeted “My cousin in Trinidad won’t get the vaccine cuz his friend got it & became impotent. His testicles became swollen”, something confirmed by VAERS reports. Steve Kirsch compiled further evidence of testicular swelling as an adverse effect of the covid vaccines.
She of course got ruthlessly pilloried for daring to claim something so obviously ‘absurd’.
And let’s not forget either the bombshell Israeli study showing significant declines in a critical sperm characteristics that have ominous implications for male fertility. Which we also don’t quite understand either.
Anything covid can do, the vaccines can do better.
************************
I finally have someone helping me cataloging the case reports :). I hope to complete a few more articles about case report ‘anomalies’ in the next week or so.
Resisting the Intellectual Illiteratti is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.
















Good point on the stigma associated with this in young men and why it may be vastly underreported.
A systemic poison oak reaction will swell the penis and testicles as well. Guess how I found out...