


Updated: Vermont's Mysterious Spike in Cardiogenic Shock Deaths of 2021
#ShockShot??

One of the starkest anomalies observable in the Vermont death certificates is cardiogenic shock deaths.
What is cardiogenic shock?
According to the NIH, “Cardiogenic shock, also known as cardiac shock, happens when your heart cannot pump enough blood and oxygen to the brain and other vital organs.”
In other words, the heart is too damaged to pump enough blood around to the entire body to keep critical organs alive.
Overview of Cardiogenic Shock Deaths in Vermont
Here are a series of charts that present a fairly comprehensive picture of deaths involving cardiogenic shock:
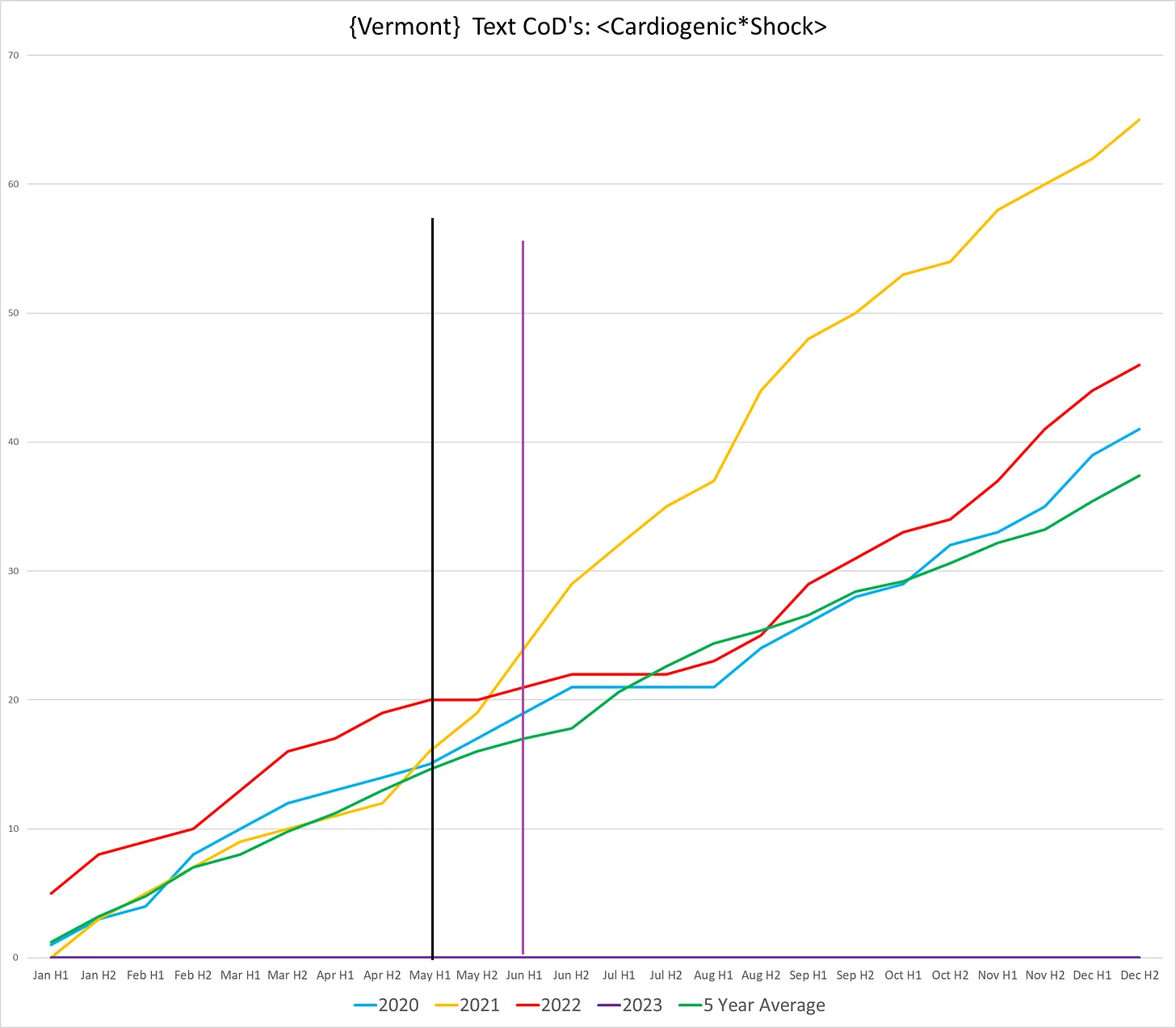
Chart #1: Total number of deaths involving cardiogenic shock, full calendar year:
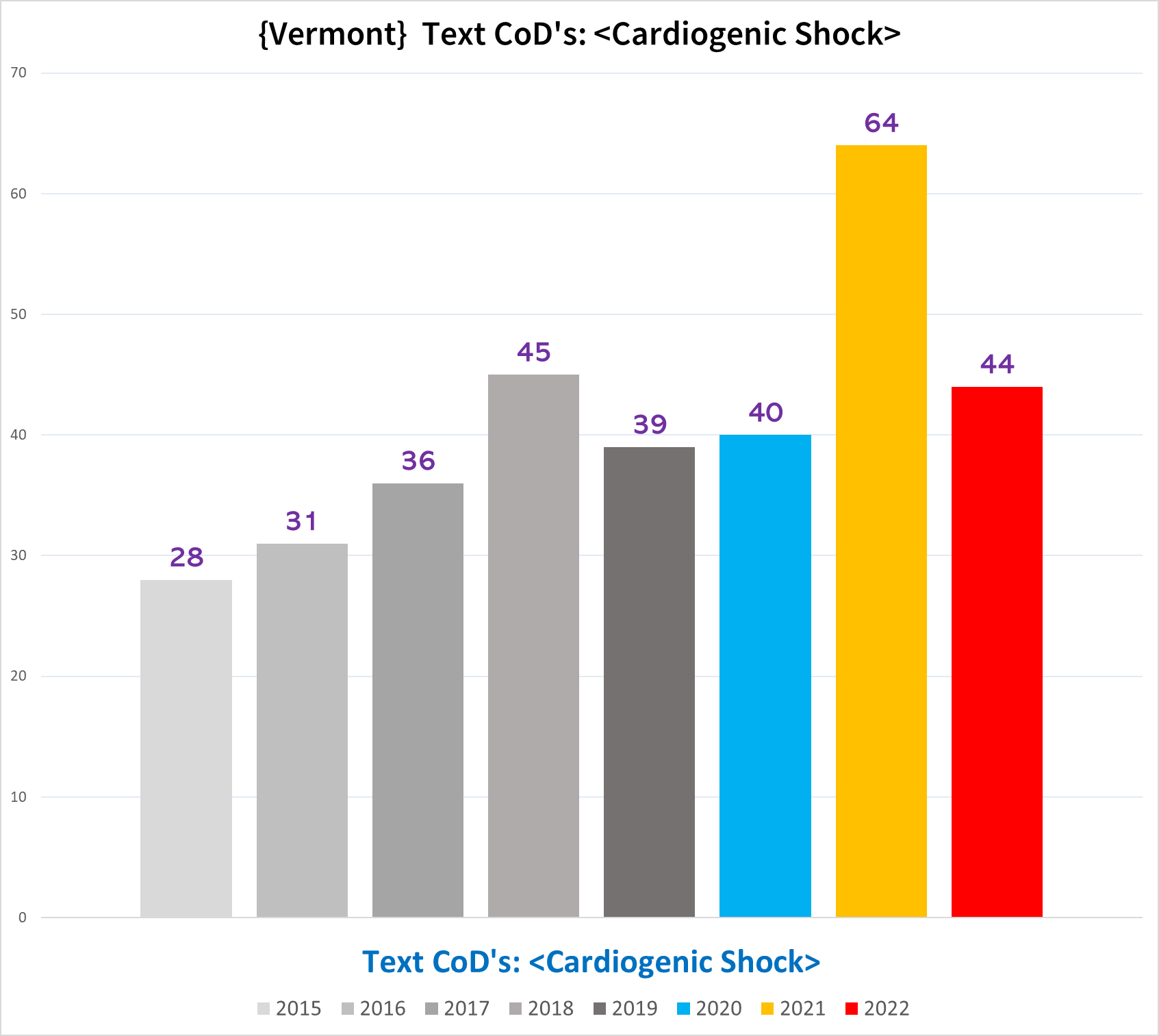
Chart #2: Total # of cardiogenic shock deaths per quarter
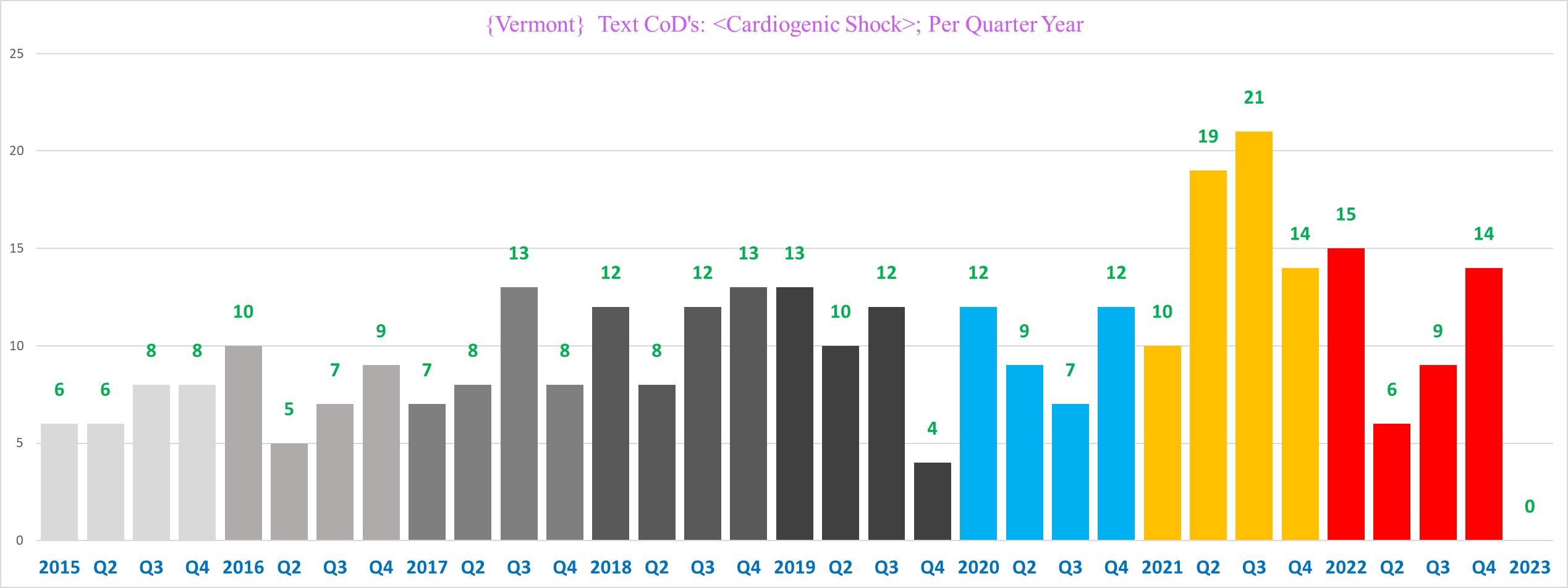
Chart #3: Breakdown of cardiogenic shock deaths in Part 1 of death certificate (left) vs in Part 2 (right):

Chart #4: Average age of cardiogenic shock deaths by year
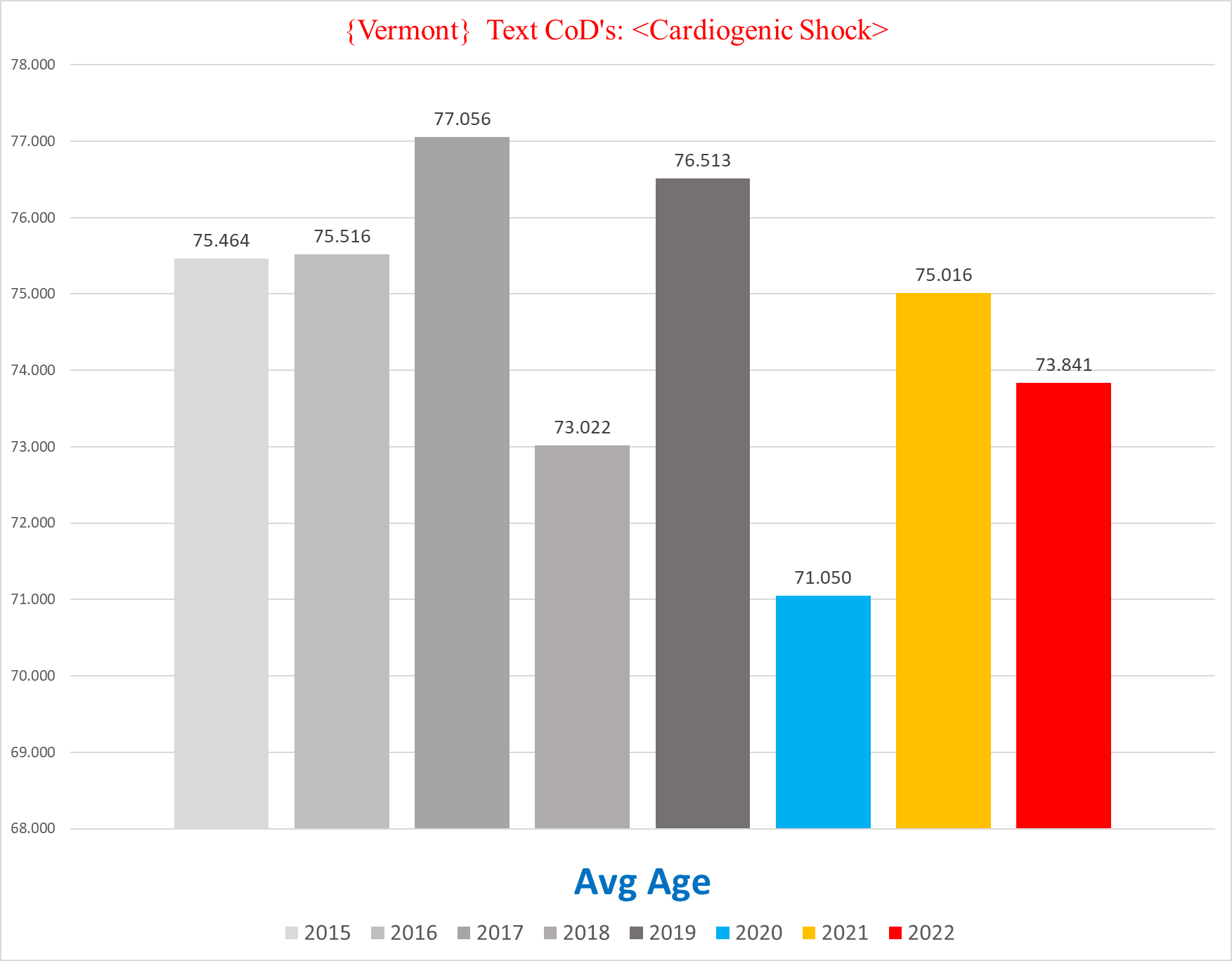
Chart #5: % of cardiogenic shock deaths by gender

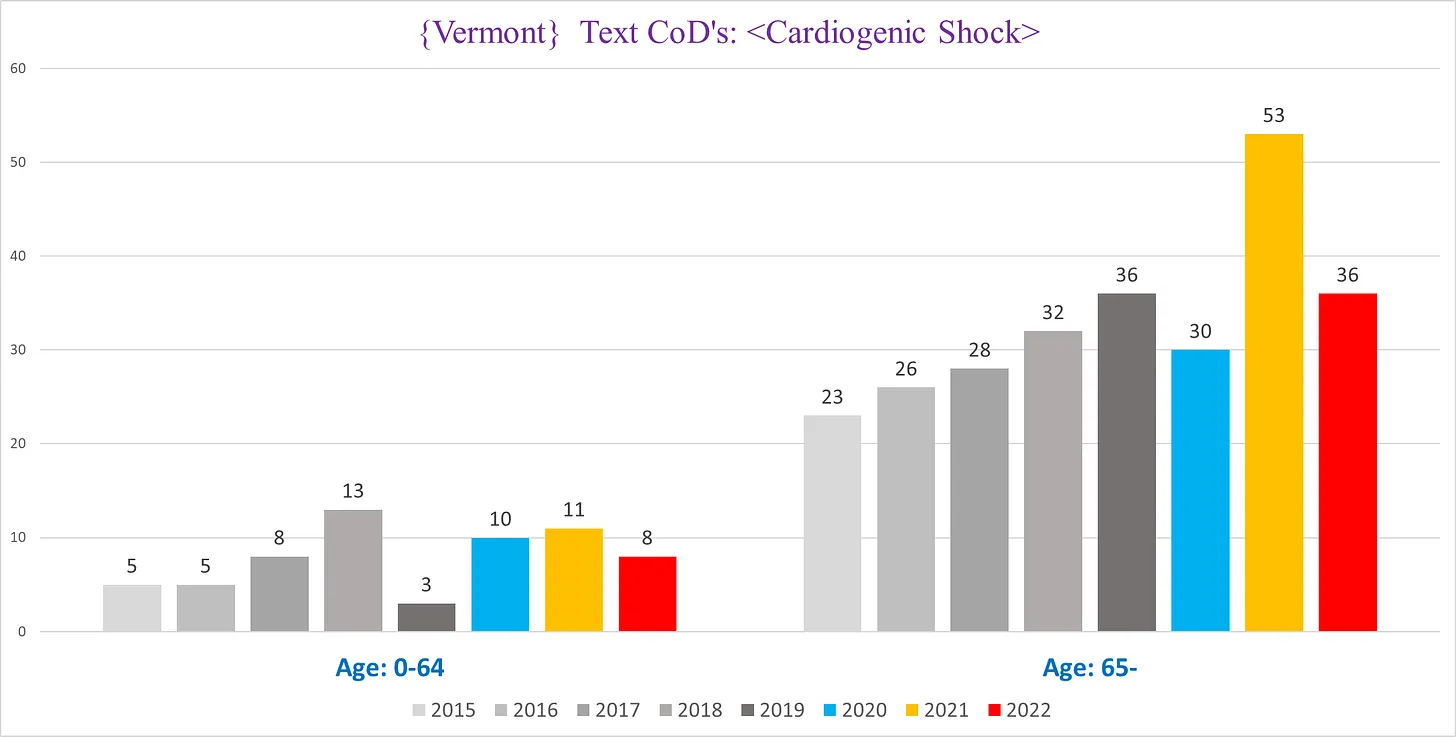
Chart #6: Breakdown of cardiogenic shock deaths by age cohort
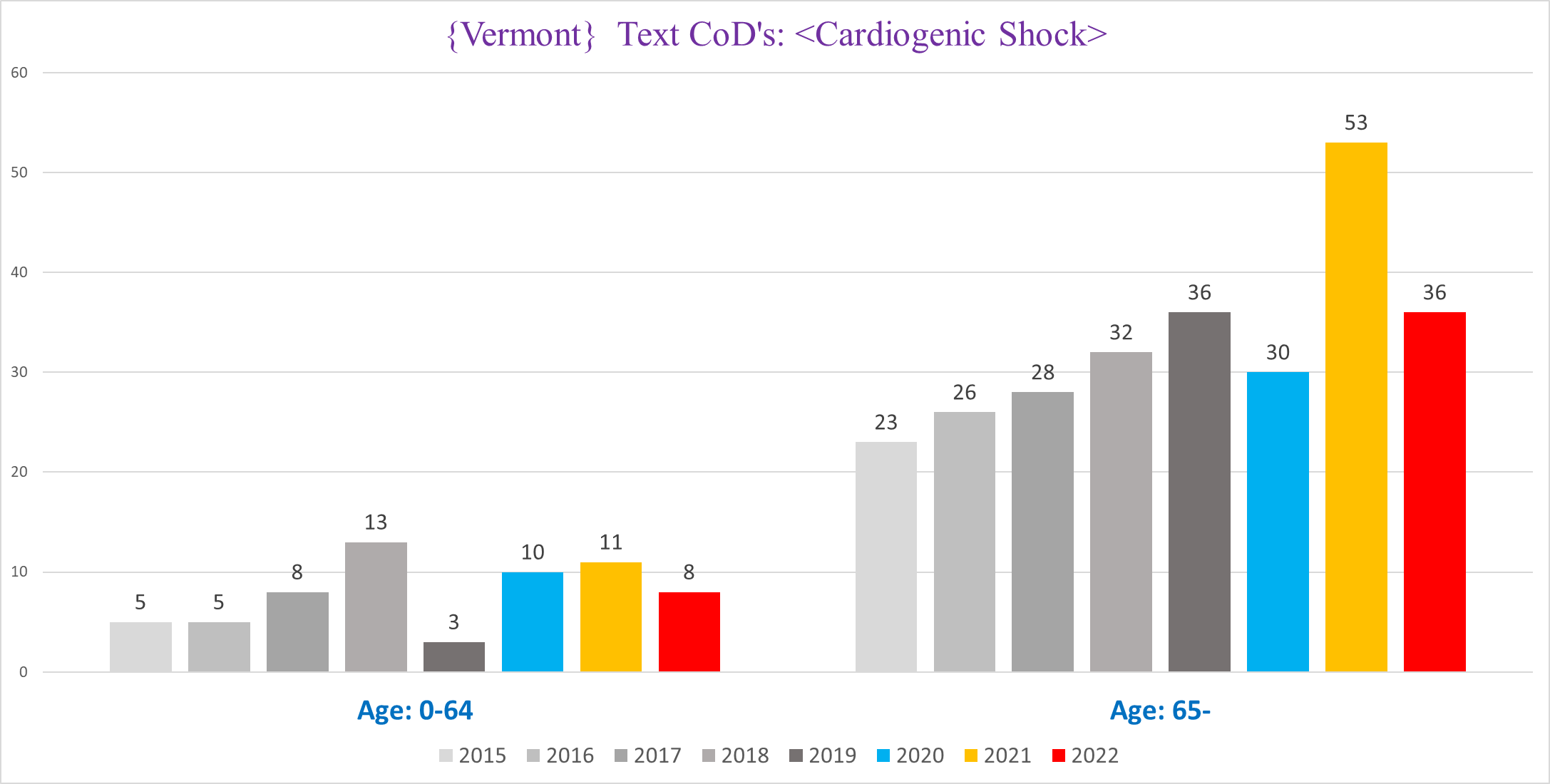

Chart #7: Breakdown of cardiogenic shock deaths by place of death and gender

Analysis
Something happened in 2021 that caused cardiogenic shocks to soar. The question is WHY.
Are the excess cardiogenic shock deaths of 2021 a clinical or administrative phenomenon?
The first thing we must determine is what the increase in cardiogenic shock deaths represents - does it reflect a change in the clinical causes of death, or is it an artifact of a shift in how ME’s/attending physicians assigned a CoD (what I am referring to as an “administrative phenomenon”)? This is not merely an abstract hypothetical question - death certificates are notoriously inaccurate and subject to widely varying conventions and degrees of competence by those who fill them out. We can attempt to adjudicate this by looking at the characteristics of cardiogenic shock deaths, to see if they are inconsistent with this trend being a clinical or administrative phenomenon.
Exhibit A: Cardiogenic shock is a CoD that is exclusive to hospital deaths:
Why would a fairly general CoD - one that would seem to be applicable to deaths outside a hospital as much as inside a hospital - only be diagnosed and/or documented in a hospital? Cardiac arrests - a very similar if not identical pathology from an ‘administrative’ perspective (and one that often is the result of cardiogenic shock) - are frequently documented on death certificates outside of hospitals:

(There is a clear signal of excess mortality in cardiac arrests, which will be the subject of an upcoming post.)
It is highly dubious that ME’s discriminate against non-hospital deaths exclusively when it comes to cardiogenic shock.
This implies that cardiogenic shock is not a diagnosis of conjecture - something that an ME would put on a death certificate as an ‘educated guess’ - but rather is a diagnosis confirmed by a clinical test or examination.
Indeed, if we look at the NIH page cited above, we find the following:
To diagnose cardiogenic shock, a catheter (tube) may be placed in the lung artery (right heart catheterization). Tests may show that blood is backing up into the lungs and the heart is not pumping well.
Tests include:
Cardiac catheterization
Chest x-ray
Coronary angiography
Echocardiogram
Electrocardiogram
Nuclear scan of the heart
I asked a few health care providers sporting various credentials about diagnosing cardiogenic shock, and there was a general consensus that it is something that is easily, accurately and reliably diagnosed in a hospital setting.
(It is plausible that cardiogenic shock would only be diagnosed in a hospital setting, because hospitals are uniquely disposed to testing for and confirming a diagnosis of cardiogenic shock -- they interdict patients while they are still alive (however fleeting that may last); they have all the patients hooked up to vital sign monitors; and healthcare personnel check in on patients more frequently than they do in nursing homes, hospices, and at the decedent’s house.
This suggests that the spike in cardiogenic shock deaths in 2021 is a clinical phenomenon reflecting a spike of a specific pathology killing people.
Exhibit B: The inversion of the gender breakdown
In the 5 years before the pandemic, cardiogenic shock was dominated by women (black lines); whereas in 2021 & 2022 (besides for 2018), the men absolutely dominate:
The one pre-pandemic year where the men have more cardiogenic shocks than the women is 2017, which saw excess cardiogenic shocks solely in men - as you can see in the below chart, while women are essentially flat, men in 2017 have almost 100% excess cardiogenic shock excess deaths - double the expected cardiogenic shock mortality - and explode in 2021:
Is it plausible that this gender-specific trend could be the product of subjective standards or decisions by ME’s or bureaucratic diktat? I doubt it. If there were a shift in how CoD’s were being assigned or diagnosed, it should show up in both genders, especially for a CoD that is distributed pretty evenly overall between both genders.
It is far more plausible that the excess cardiogenic shock deaths in men reflect the increase in a pathology/s appearing in hospital decedents.
Ergo, it is reasonable to presume that the excess cardiogenic shock deaths are capturing a real clinical phenomenon of unexpected excess deaths caused by a pathology/s that results in cardiogenic shock.
What is causing the increase in deaths caused by or involving cardiogenic shock?
Since we can reasonably assume that there is indeed a genuine increase in fatal cardiogenic shocks, we can now try and see if we can figure out what is causing this increase, or at least rule out potential hypotheses.
Timing
The most salient characteristic relevant to figuring out what can or cannot be responsible for this trend is when did it occur. Obviously, if ‘A’ caused ‘B’, it has to fit chronologically. If there is little or no discernable relationship between the occurrence of ‘A’ and ‘B’, it is unlikely that ‘A’ is causing ‘B’.
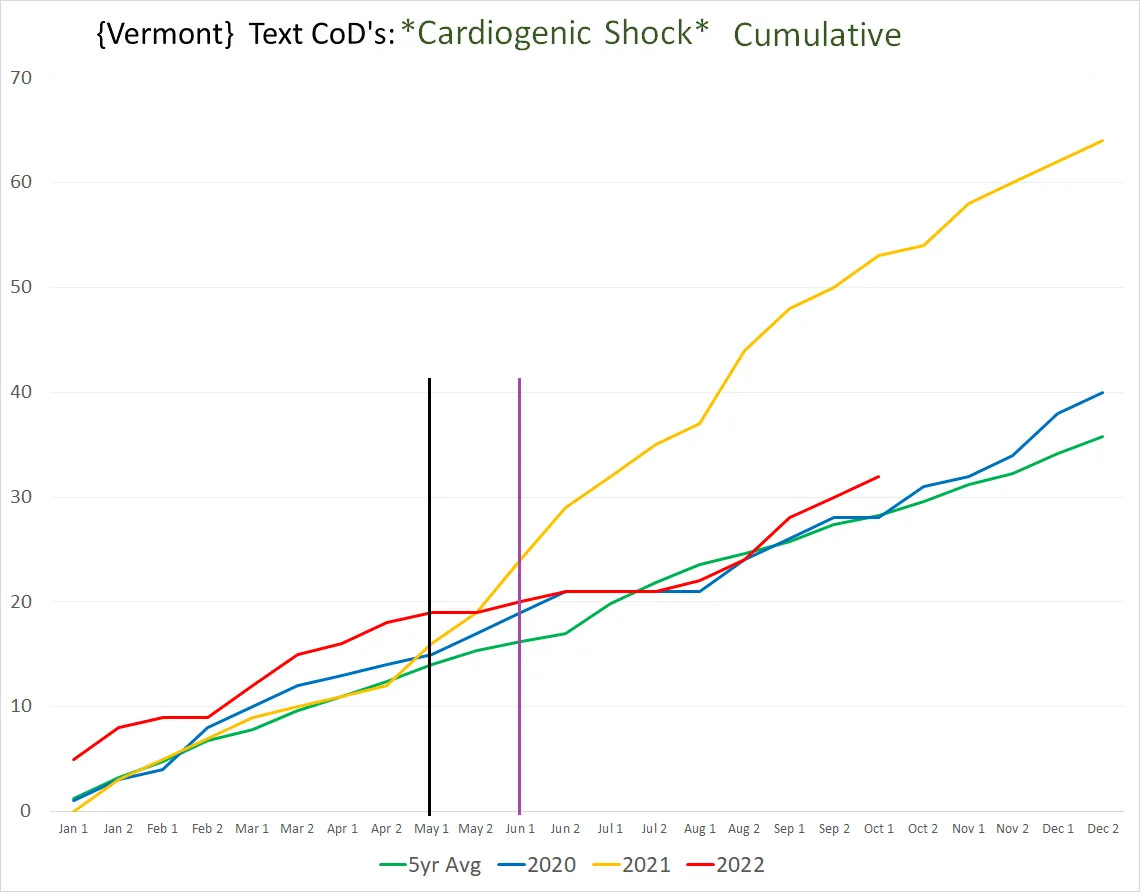
Here is the trendline of cumulative cardiogenic shock deaths (black vertical line indicates where the trend starts to deviate from the pre-pandemic average; purple vertical line indicates where it starts to surge):
Can this be explained by covid?
We can safely rule out covid from contention here:
Covid was around in 2020, including a significant winter 2020/21 wave, yet there was no surge in cardiogenic shock deaths.
There was only ONE death that listed both covid *and* cardiogenic shock in 2020, and only TWO such deaths in 2021.
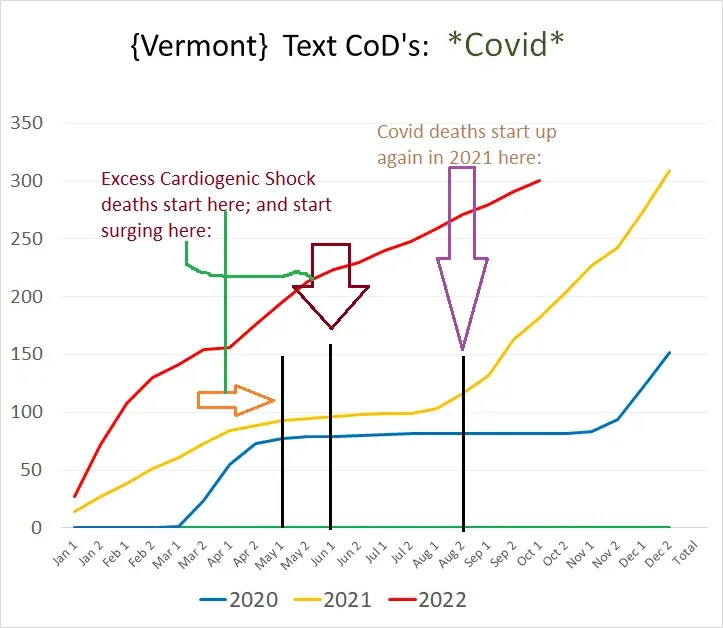
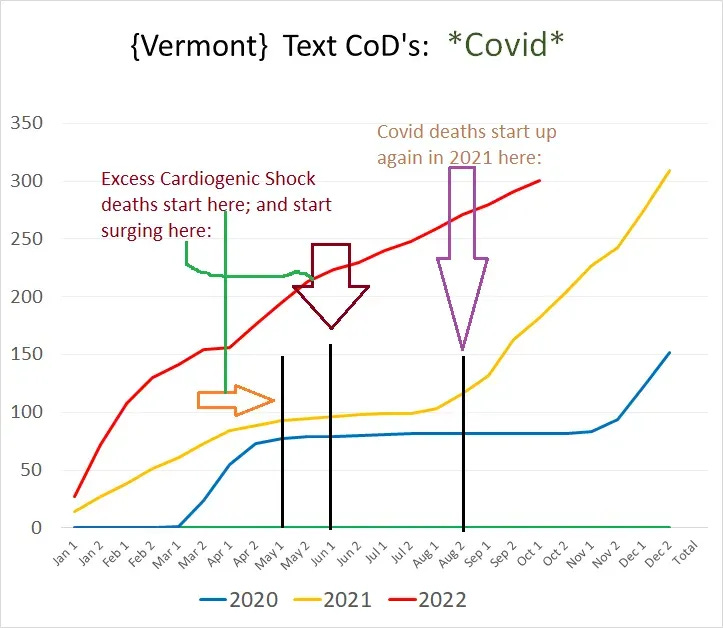
The surge does not coincide with any covid wave - it falls smack in the middle of the lull between the 2020 winter wave and the 2021 fall surge in covid deaths, where there were practically no covid deaths over the span of about three months, visualized in the chart below showing the cumulative # of covid deaths by half-month intervals:
This cannot plausibly be chalked up to long covid either - long covid would not cause a sudden, massive surge first starting a full 15-18 months after covid began spreading around the US. Furthermore, the cardiogenic shock curve does not match any covid trend in Vermont, even one offset by 15 months.
Can this be explained by the covid vaccines?
If you look at where this trend begins, it mirrors vaccine uptake offset by about 5 months - slow start for a few weeks as vaccines were in very short supply but picking up afterwards as vaccines became more readily available and deployed:
The bump
Cardiogenic shock is almost exclusively in the senior population - who were overwhelmingly the recipients of the vaccines at the start of the vaccine rollouts - (and there was only *ONE* cardiogenic shock death under the age of 40):
There is a credible hypothesis that a subset of vaccine deaths take a few months to manifest, which lines up perfectly with Vermont's trend of cardiogenic shock excess deaths that kicks off about 5 months after the vaccines were first introduced.
For instance, a case series from a Japanese cardiologist’s practice also found an increase in cardiac deaths spread out over the following months:
Subacute Effects of Vaccination with a Messenger RNA-based Vaccine Against Coronavirus Disease 2019 on Elderly Japanese Patients with Cardiac Disorder
https://www.researchsquare.com/article/rs-1391307/v1
I previously wrote about this study on substack:

Cardiogenic shock was a part of the pathology directly causing the death
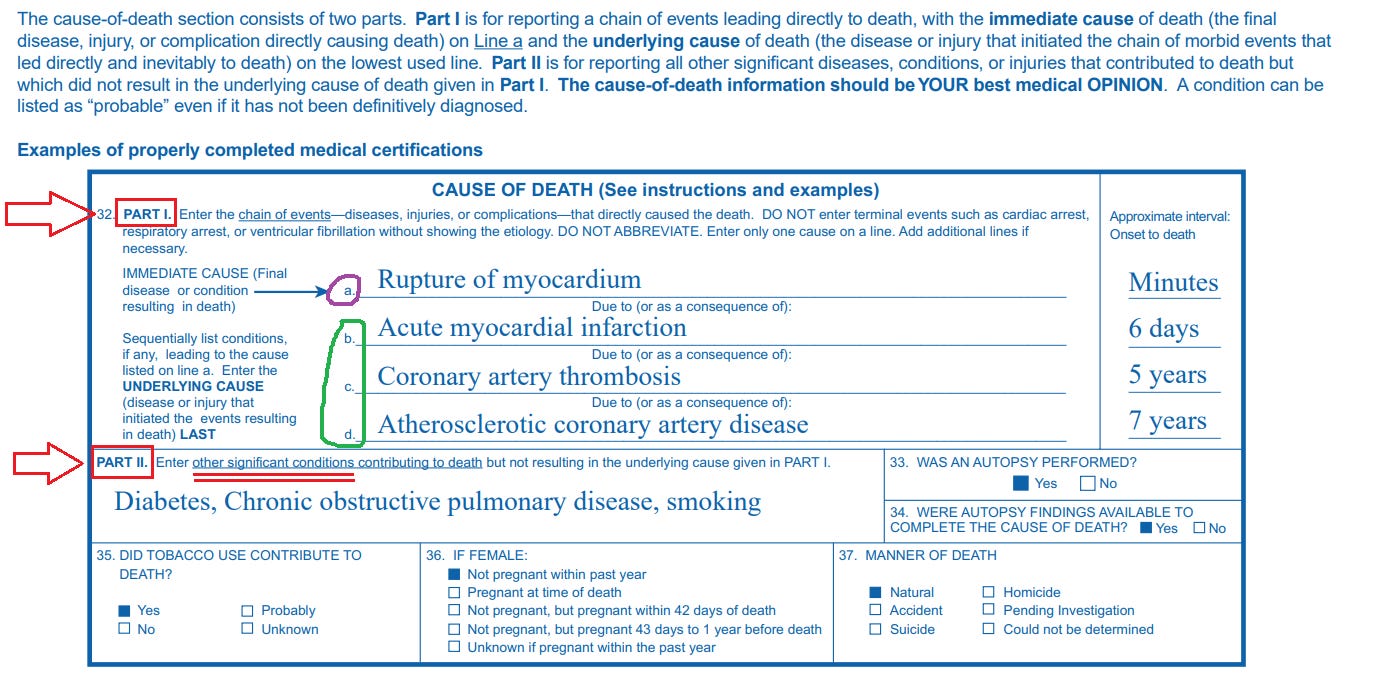
One of the notable characteristics of the excess cardiogenic shock deaths is that they almost all appear on Part 1 of the death certificate (left chart shows the total # of cardiogenic shock deaths where the cardiogenic shock is in Part 1; right shows where it is in Part 2):
Clearly, cardiogenic shock is almost exclusively a “Part 1 CoD”.
Part 1 of the death certificate is for the “chain of events leading directly to death”; and Part 2 of the death certificate is for “all other significant conditions” (screenshot below from CDC guidance on filling out death certificates):
Thus the excess cardiogenic shock deaths in Vermont in 2021 are capturing a clinical phenomenon of something causing an increase in the number of patients who suffered a fatal event of cardiogenic shock.
We know that the covid vaccines can cause cardiogenic shock. Additionally, cardiogenic shock itself can be precipitated by myocarditis, which is probably the most prominently associated adverse pathology of the covid vaccines. And although covid vaccine-associated myocarditis has been more commonly documented in younger people, it has also been documented in seniors. Thus it is also possible that this excess cardiogenic shock is hiding undiagnosed cases of vaccine-associated myo/pericarditis in seniors.
For example, the following case report study documents a case of myocarditis leading to cardiogenic shock in an octogenarian woman within days of receiving a Pfizer vaccine:
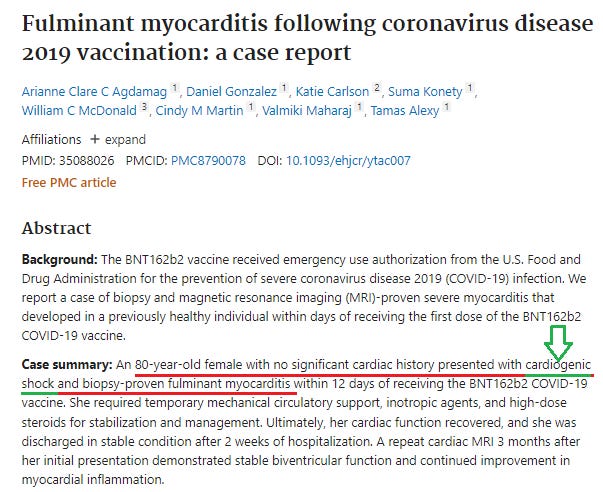
This is just one from among the bevy of case report studies documenting covid vaccine-associated cardiogenic shock:

It is further plausible that ‘mild’ or subclinical manifestation of myocarditis can be fatal for seniors even though it’s not typically fatal in the short-term for younger people. Unlike younger people, seniors are far less likely to be able to withstand even ‘mild’ (i.e. a small amount of) heart inflammation. If you’re young and healthy, then losing a bit of cardiac output or function in itself probably isn’t going to kill you in the short or mid term (although a sudden arrhythmia from the disruption of electrical signaling by scar tissue might). On the other hand, a 77 year old man with five conditions does not have ‘spare’ cardiac function that he can lose and still survive, so a bit of ‘mild’ myocarditis (and for sure a nice, big splotch of myocardial or pericardial inflammation) can eventually reduce cardiac function below the minimum necessary to survive.
In the current political and social climate post-vaccine rollout, hospitals would rather not figure out the underlying cause of heart damage, and are therefore incentivized to leave diagnosed heart damage as simply that - something that could easily be diagnostically captured as ‘just an unfortunate case of cardiogenic shock’. “Myocarditis only affects young males” has been one of the public health establishment’s critical go-to talking points used to discount and disrepute any data showing widespread cardiovascular carnage from the vaccines to all age groups and demographic cohorts, one that they can ill afford to lose.
‘Seeing through’ a pull-forward effect
There is a further point in this vein that is worth fleshing out a little.
One of the biggest confounders in discerning excess mortality in 2021 and 2022 is the “pull-forward” effect.
A substantial increase in a defined clinical condition or pathology however can rise above this to some extent, because we are able to identify a definite excess in the excess deaths from this specific condition, regardless of the total nominal number of deaths. Obviously, this is not by itself conclusive proof of anything, but as part of a broader mosaic of evidence and data, it is helpful to better pinpointing or clarifying what and where the excesses we are seeing in various data are.
Caveats
There are several important caveats to this analysis that must be stipulated.
Small sample size
Although the signal is large enough that it cannot be written off to random chance, it is way too small to definitively prove anything specific. Vermont only had 6,685 deaths total in 2022, and that includes the excess. That notwithstanding, it jives well with a lot of other evidence and observations about the devastation wrought by the covid vaccines.
Subjective and/or arbitrary nature of death certificates
Death certificates are notoriously fickle, error prone, and rife with inaccuracies. It is possible that there are other ‘administrative’ variables in play here affecting how CoD’s are being designated.
The totality of cardiac related deaths
I have noticed that there seems to be some degree of interchangeability between the various conditions of some organ systems or disease. For instance, there seems to be some amount of balancing out between ‘embolism’ and ‘thrombosis’ - they fluctuate somewhat year to year but combined they even out.
If there is a decrease in other types of cardiac deaths corresponding to the increase in cardiogenic shock deaths, then the most likely interpretation is that cardiac deaths that would usually be documented as a cardiac arrest for instance are instead for whatever reason being documented as cardiogenic shock.
However, here deaths involving other cardiac conditions in Vermont do not decrease while the cardiogenic shock deaths increase, so the excess cardiogenic shock deaths cannot be attributed to simply labelling other cardiac-related deaths as cardiogenic shock.
In a nutshell, there was an obvious spike in deaths involving cardiogenic shock in 2021 in Vermont.
The fact that every single death but one occurred in a hospital, and that the excess occurred almost exclusively in men, suggests that this trend is not the product of human decisions or arbitrary changes in CoD adjudication conventions, but rather reflects a genuine clinical phenomenon of an unanticipated excess mortality associated with heart damage captured by a diagnosis of cardiogenic shock.
Moreover, while the timing of the excess cardiogenic deaths suggests that it is implausible to attribute them to covid, long covid, or the consequence of some other pandemic policy, it is not inconsistent with the covid vaccine rollout.
Finally, there is a plausible mechanistic basis to support the hypothesis that these excess deaths were ultimately caused by a pathology initiated by a covid vaccine.
More COVID vaccine excess deaths-related data on top of mountains of similar irrefutable mortality data - some revealed and much hidden - all pointing to a growing herd of elephants in the room. Getting hard to ignore these but the culpable are relying on our becoming numb or surrendering to the official “Trust The Science” wall of silence. Should be sufficient cause to initiate legal proceedings I would think. Personally, I would not stand by or forget if a loved one passed away in this manner!
One of the most jabbed states by some account I read recently. It made me reconsider ever moving there.