
Case Report Study from cardiologist shows 38% of patients with pre-existing subclinical heart failure either died or experienced dramatic worsening of their heart failure following vaccination
Authors proposed that "autoimmune myocarditis is the most likely explanation"

Bullet point summary:
Japanese cardiologist published a study documenting his own experience with vaccinated patients
Patients ages ranged from 78-89.5 & only 45% were male - these were *not* young men
21/55 (38%) of patients with pre-existing subclinical heart failure [defined as BNP ratio 4x normal upper limit] either died (6) or suffered dramatic worsening of heart failure (15) 1-8 months after vaccination
0/45 patients with BNP <4x the normal upper limit died or suffered worsening heart failure [defined as an increase in BNP ratio equivalent to at least 10x their baseline BNP ratio post vaccination compared to pre-vaccination] in the 1-8 months following vaccination
The death rate in his practice over the preceding 4 years was 5-7%
The death rate in his patients during the first six months of the time period covered by the study was double the historical rate - 13.7%
Authors proposed that the “most likely explanation is autoimmune myocarditis”
What the study did/found (in English)
A Japanese cardiologist had treated a lot of seniors in Japan, many of whom had been vaccinated, which provided an opportunity to see if there were cardiac adverse events following vaccination.
(They published a follow-up longer term study that will be the subject of a separate substack article.)
He together with a bunch of number-cruncher scientists published a study a while back documenting a bunch of heart failures and deaths in some of his patients:
Subacute Effects of Vaccination with a Messenger RNA-based Vaccine Against Coronavirus Disease 2019 on Elderly Japanese Patients with Cardiac Disorder
https://www.researchsquare.com/article/rs-1391307/v1
(I am not surprised the peer review process seems to be dragging its feet on this one.)
Here’s how he described his experience (in the original study):
Six and 15 patients expired and exhibited significant increment of the BNP ratio, respectively; these patients had a pre-BNP ratio ≥ 4-fold higher than the UNL. Forty-five patients with a pre-BNP ratio < 4-fold higher than the UNL did not expire or show significant increase in the BNP ratio. The pre-BNP ratio was a reliable parameter for predicting cardiac deterioration after vaccination. For the booster or initial vaccination against COVID-19, the BNP ratio may be useful in assessing the cardiac status of elderly patients.
The degree of increase after vaccination (i.e., post-BNP ratio minus pre-BNP ratio) was significantly high (≥ 10-fold higher than their UNL) in five patients who expired and 15 patients who survived. Death and/or remarkable increase in the BNP ratio (i.e., ≥ 10-fold higher than the UNL) were observed only in patients with a pre-BNP ratio ≥ 4-fold higher than the UNL (21/55, 38.2%) (Table 2). In contrast, 45 patients with a pre-BNP ratio < 4-fold higher than the UNL in the pre-vaccination period did not expire or show remarkable increase in the BNP ratio (0/45, 0%) (Table 2). Hence, the pre-BNP ratio was a reliable parameter for predicting cardiac deterioration 1–8 months after vaccination [].
In plain English, 21 of his 55, or 38% (!!) of his patients with a high BNP ratio pre-vaccination (basically a way of quantifying a certain biomarker indicative of heart failure) either died or suffered worsening heart failure in the 8 months following vaccination, whereas none of his 45 patients with a low BNP ratio pre-vaccination died or suffered worsening heart failure post-vaccination.
They concluded as follows:
This study showed that vaccination against COVID-19 was associated with a high risk of death or decompensated heart failure for Japanese elderly patients with severe cardiac dysfunction and a high pre-BNP ratio ≥ 4-fold higher than the UNL (500 ng/mL in NT-pro BNP). However, the risk was negligible in patients with a pre-BNP ratio < 4-fold higher than the UNL (Table 2). The incidence of death and/or remarkable increase in the BNP ratio (i.e., ≥ 10-fold higher than the UNL) in the post-vaccination period was strongly dependent on a pre-BNP ratio ≥ 4-fold higher that the UNL (500 ng/mL in NT-pro BNP in Table 2). Cardiovascular death after the vaccination developed only in patients with a pre-BNP ratio > 12.6-fold higher than the UNL (1,575 in NT-pro BNP). Patients with a pre-BNP ratio < 4-fold higher than the UNL in the pre-vaccination period did not expire or show remarkable increase in the BNP ratio after vaccination. This cardiac deterioration was not accompanied by side effects, such as anaphylactic hemodynamic deterioration or sustained high fever in the acute phase, or myocardial infarction, liver dysfunction, or renal dysfunction (Table 1) both in the acute and subacute phases.
This study offers a very critical insight. People have a tendency to dismiss the covid vaccine as a potential cause of death in patients with pre-existing conditions. Yet, this study highlights that it is precisely in the patients with pre-existing disease that the covid vaccines are particularly dangerous.
Myocarditis?
The authors proposed that the most likely explanation for the observed cardiac side effects was that the covid vaccine triggered an autoimmune myocarditis:
The most likely explanation for this sustained myocardial involvement in the subacute phase would be autoimmune myocarditis; in other words, anti-idiotype antibodies-dependent myocarditis recently proposed by Murphy and Longo.5,6 The primary antibody induced by vaccination against COVID-19 has antigen-binding domains with a mirror image structure of the spike protein of COVID-19. Hence, it may induce a secondary antibody with a mirror image structure of the antigen-binding domains of the primary antibody. Consequently, the secondary antibodies may be able to bind to the angiotensin-converting enzyme 2 (ACE2) receptor as the spike protein of COVID-19, thereby inducing the release of inflammatory cytokines. This hypothesis may explain our observation that myocardial dysfunction was sustained for several months after vaccination and led to the death of patients with severe damage. Nevertheless, massive myocardial necrosis was not noted. The transition of the BNP ratio suggests that myocardial damage appears to be somewhat reversible (Fig. 1C D) in certain cases, but sustained in others.
It is worth emphasizing that these were not young men - the age range here was 78-89.5, and 55% were women (!!) - but a significant % suffered what the authors suspect was autoimmune myocarditis.
Death rate during the study period was roughly double the death rate during the previous 4 years
An added strength of this study is that this cardiologist had his historical experience to serve as a control group of sorts. Whereas the death rate in his patients over the prior 4 years was about 5-7%, the death rate in his patients during the time period of the study was DOUBLE that, clocking in at *13.5%*:
The BNP and/or NT-pro BNP levels in patients with severe cardiac dysfunction may increase during the natural course of the diseases. Therefore, one may argue that the increase in the BNP ratio after vaccination may be caused by the natural course of the diseases. However, in the previous 4 years, the cardiac death rate every 6 months among patients treated by the corresponding author at home or care facilities was 5.0–7.1% (seven terms). This was accompanied by a maximum BNP ratio ranging 12.6–280-fold higher than the UNL (median: 49.4; interquartile range: 29.7–103.2) and 1,575–35,000 pg/mL in NT-pro BNP (median: 6,180, interquartile range: 3,710–12,900). Nonetheless, the cardiac death rate in the previous 6 months (May 1 to October 31, 2021) was 12 cases (13.5%), including the six patients who expired after vaccination with an mRNA-based vaccine against COVID-19. The cardiac death rate among patients treated at home or care facilities who did not receive the vaccination during the same period was six cases (6.7%).
Note: The 13.5% death rate is NOT stated as the rate for *vaccinated* patients, but for ALL patients during this time span - only 6/12 deaths were vaccinated.
Deaths involving heart failure are way up in the post-vaccine era
I previously wrote about the escalating excess from heart failure in Vermont:
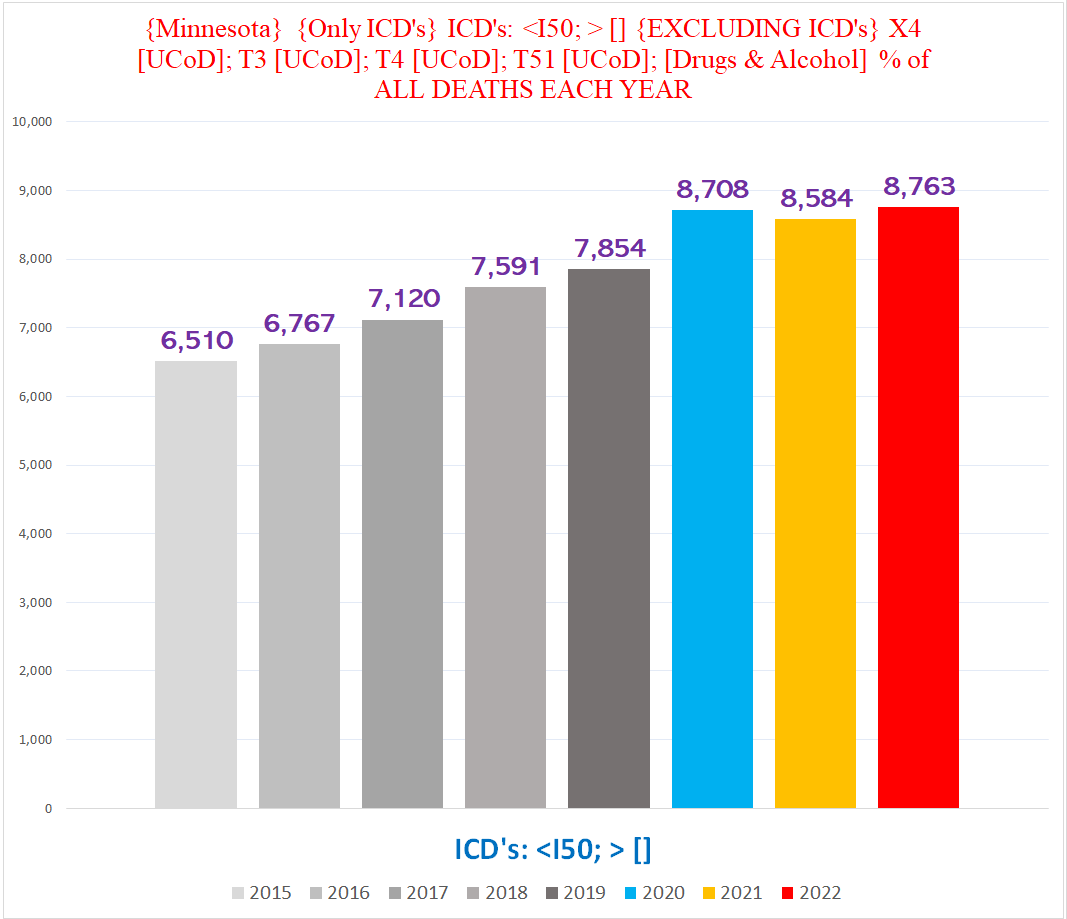
In Minnesota, deaths involving heart failure have also been skyrocketing:
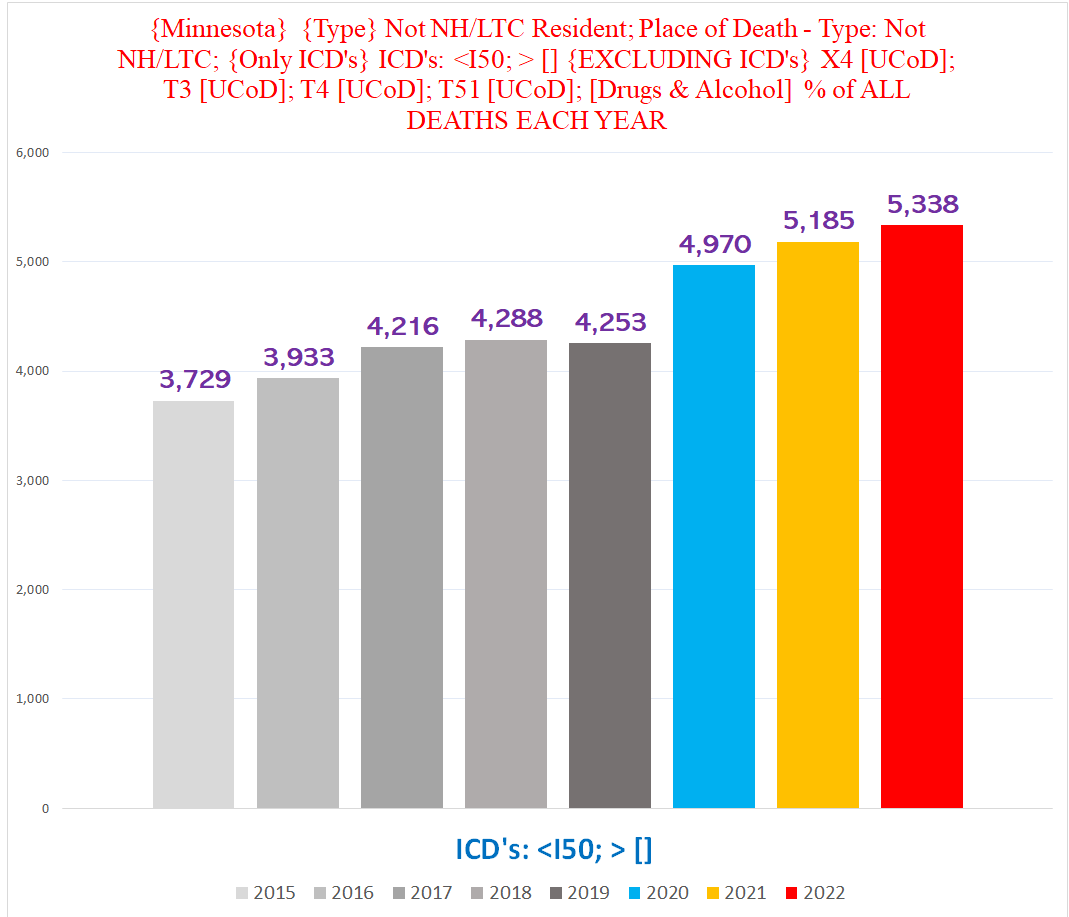
The degree of excess is even more pronounced if we exclude deaths in nursing home or LTC facility residents:
So… welcome to the new guiding principle of health:
TY for this valuable post. It should be shared far & wide! Excellent 👍 work keeping the WORLD INFORMED!
Excellent article. Thanks for the valuable information.