


What They (Allegedly) Didn't Know About the Vaccines - Summarizing the Mechanistic Pathways by Which the Vaccines can Cause Harm
A list of legitimate concerns with the covid vaccines to show your local pro-vaccine doctor

Surprisingly, I still hear a lot of “there is no plausible mechanism that can explain the covid vaccines causing _____”. To attempt to help remedy this, here is a comprehensive review touching on most if not all of the myriad ways the genetic covid vaccines can cause problems.
While this is going to get somewhat technical, it doesn’t matter if you grasp all of the nuance. This is just an attempt to pull together the various categories under which the myriad different potential vaccine induced harms can be sorted into. This is only intended to highlight the aspects of the vaccines that are problematic, not engage in a thorough analysis explaining the technical scientific rationale behind them. You can show this to your local doctor even if you don’t understand any of it - if he or she is hawking the vaccines, then he or she should be able to understand and explain it to you.
To quickly summarize how the vaccines work: mRNA that encodes for the full length spike protein of the original Wuhan strain (with a few minor alterations), packed inside lipid nanoparticles (LNP), is injected in a suspension (the liquid). The LNP’s ferry the mRNA into cells where they temporarily hijack parts of the cell’s “machinery” (primarily the ribosomes) that read/translate genetic code to produce proteins to produce the covid spike protein instead of the normal human cell proteins. The spike proteins, after being synthesized and folding into their proper shape, “swim” up to the surface of the cell where they protrude out of the cell’s membrane. Weird, protruding spike proteins on what should be healthy cells are spotted by circulating immune cells and identified as ‘foreign’, which leads to the immune system activating a broad range of mechanisms to deal with the ‘enemy’ spike proteins. The final result of the immune activation is the production of immune cells, such as antibodies and B- & T- Cells, that recognize, bind and/or neutralize covid spike proteins, which will be ready and waiting to quickly neutralize a covid infection should it subsequently occur.
After all, isn’t this how vaccines typically work, so what can possibly go wrong?
Quite a bit, actually.
Vaccine Components
There were many tactical design choices made in creating the genetic covid vaccines, which turned out to have significant implications for safety and efficacy (although you wouldn’t realize this from the language bandied about by everyone discussing the vaccines that makes them sound like the most simple and straightforward drugs ever made).
(Obviously, the most impactful decision made by the vaccine designers was choosing the spike protein as the part of the virus to use for the vaccine effect. We’ll get to this later.)
Lipid NanoParticles (LNP’s)
The vaccines utilize a LNP as the packaging and delivery vehicle to get the mRNA inside of the human cells. These LNP’s are actually a combination of different lipid compounds.
The LNP’s have several alarming or unknown characteristics that were not adequately studied (if at all). Had the basic safety standards for new biological products been followed, none of these would be unresolved or problematic:
Firstly, nanoparticles in themselves can be harmful, especially for sensitive organs like reproductive tissues, such as what is documented in the study Potential adverse effects of nanoparticles on the reproductive system.
The LNP’s used are highly inflammatory. Inflammation is a destructive mechanism used by the immune system to kill invading pathogens and diseased tissue, not something that you want to randomly provoke anywhere in the body where the LNP’s end up. A particularly concerning characteristic documented by the study The mRNA-LNP platform's lipid nanoparticle component used in preclinical vaccine studies is highly inflammatory is that the LNP’s “activate multiple inflammatory pathways and induce IL-1β and IL-6 [interluekin-6]”. (IL-6 is the worst of the covid-19 cytokine storm’s cytokines.)
In order to get the LNP’s to properly bind with the mRNA strands, it was necessary to employ cationic lipids - lipids with a positive electrical charge. Cationic lipids are known to be toxic. for instance, Lipid-Based Nanocarriers for RNA Delivery reports that “[a] cationic lipid molecule can disrupt the integrity of a membrane structure as it resembles a detergent. At low concentration, a lipoplex consisting of cationic lipid molecules can irritate the exposed cell and cause cytoplasm vacuolization, reduced number of mitoses and cell shrinkage.”
Naturally, the LNP formulations used in the Pfizer and Moderna vaccines were not tested (at least not in any documentation available to the public) to see if the chemistry “fix” (an ionizable cationic lipid that would have a neutral charge at a neutral PH) would hold up or not cause a new set of unintended consequences.
One of the lipid compounds used is contains PEG (Polyethylene Glycol). As Dr. Byram Bridle pointed out in his expert report to a Canadian court, “C57BL/6 mice were administered an intra-ocular injection of PEG8 to induce choroid neovascularization (CNV) after complement activation (Polyethylene glycol (PEG)-induced mouse model of choroidal neovascularization), and may serve as a model for studying macular degeneration of the retina. Dutch belted rabbits injected with PEG400 were reported to have retinal degeneration and atrophy 5 days post injection (Retinal Toxicity of Polyethylene Glycol (PEG)-400). Both of these studies demonstrate that small sized PEGs were found to be toxic [].”
Dr. Bridle goes on to observe that “PEGs were thought to have inert characteristics. However, it is now widely appreciated that they possess
potent immunogenic properties. Exposure to PEG can result in the production of anti-PEG immunoglobulin (Ig)M and IgG, which can activate the complement system and result in anaphylaxis.”How the LNP’s are metabolized, and what compounds the LNP’s degrade into, are not adequately characterized.
The efficiency and reliability of commercial manufacturing processes used to make the LNP’s and put them together with the mRNA is not verifiable through publicly available documentation, to say the least. And no, a manufacturing company issuing a statement does not constitute ‘documentation’ that ‘verifies’ anything. (Fun fact: the LNP is actually created by making a sort of big chemical soup where the various lipid compounds “self-assemble” around mRNA strands.) We’ll explore the manufacturing process more later on.
mRNA
mRNA is not a monolithic entity. There is a tremendous amount of delicate nuance in the design of mRNA molecules. (For the academically adventurous, Engineering of the current nucleoside-modified mRNA-LNP vaccines against SARS-CoV-2 does a decent job of explaining the mRNA vaccine architecture.) The mRNA used by the vaccines actually is radically different in some respects from ‘normal’ mRNA made and used by human cells, which give rise to a host of potential complications from unanticipated or unforeseen biological chemistry:
Substitute Nucleotide N1-Methylpseudouridine - The vaccine mRNA use modified versions of several nucleotides (these are the “building blocks” of RNA/DNA), notably N1-Methylpseudouridine (m1Ψ) in place of Uridine, in order to enhance protein translation and avoid detection by enzymes that sense and destroy foreign RNA and help degrade typical mRNA (among other things).
The impact of m1Ψ upsetting the dynamics of the biological environments in host cells is unknown, but considering that m1Ψ significantly changes how the cell reacts to the mRNA, this concern cannot be dismissed lightly. The m1Ψ might also be responsible for runaway production of spike protein in some people (Immune imprinting, breadth of variant recognition, and germinal center response in human SARS-CoV-2 infection and vaccination found that “BNT162b2 vaccination produces IgG responses to spike and RBD at concentrations as high as those of severely ill COVID-19 patients and follows a similar time course”). This is hypothesized by Dr. Robert Malone based on the m1Ψ utility that is documented in studies like the one he cites, N 1-Methylpseudouridine substitution enhances the performance of synthetic mRNA switches in cells, or N1-methyl-pseudouridine in mRNA enhances translation through eIF2α-dependent and independent mechanisms by increasing ribosome density.
Keep in mind, it was not absolutely vital to utilize substitute nucleotides - as Dr. Malone also pointed out, “Curevac does not use pseudouridine in its formulation and it is not required or necessary for a significant immune response”, as documented in the study Optimization of non-coding regions for a non-modified mRNA COVID-19 vaccine.
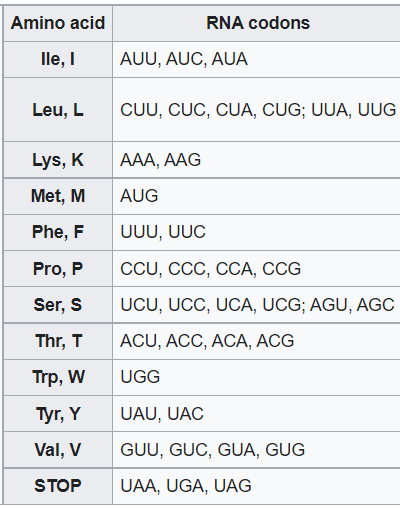
Codon Optimization - This is technically dense, but here’s the basic idea: Proteins are made up of amino acids. Amino acids are encoded by the RNA in three letter (nucleotide) sections called codons - for instance, ‘CCC’ (3 Cytosine’s) encodes for the amino acid Proline (P). Almost all amino acids have multiple codons that encode for them (STOP is the signal that you reached the end of the part of the RNA that encodes the protein itself):
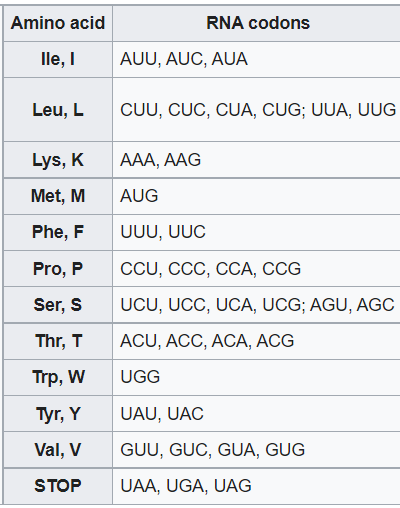
Codon optimization (for our purposes) refers to changing the codons used by the virus to codons that will ‘work better’ in human cells. The vaccine designers made liberal use of this technique. This was despite codon alterations being known to potentially cause problems, e.g. Synonymous codon substitutions perturb cotranslational protein folding in vivo and impair cell fitness. Specifically relating to the covid vaccines, Dr. Peter McCullough (and a few others) published a study exploring some of the potential negative impacts of the codon optimizations: Innate Immune Suppression by SARS-CoV-2 mRNA Vaccinations: The role of G-quadruplexes, exosomes and microRNAs.
mRNA Analogue Caps - mRNA strands are capped on the front end with a five-prime cap (5′) & on the back end with a three-prime untranslated region (3′ UTR). These regions influence or regulate various characteristics of the protein being synthesized from the strand of mRNA - sort of like an instruction manual dictating the specs of how you want this protein to be made (think of a car or furniture that can be made to different specifications to fit different unique purposes). These caps are also critical to the viability and quality of the mRNA - as one manufacturer puts it, “Proper mRNA capping is critical to the production of the most biologically active and least immunogenic mRNA.”
Naturally, the vaccine designers went all in and chose the most aggressive “instructions” possible - maximum translation speed, max translation efficiency (minimize translational errors), max translation quantity, among other selected “specs”. The impacts of this unnatural combination of choices is, of course, untested. Dr. McCullough with Dr. Anthony M Kyriakopoulos published a short paper touching on some of the considerations implicated by the design of the mRNA analogue caps, Does the High Binding Affinity of Analogue Caps to the elF4E Obey the Laws of Thermodynamics for Cellular Health? (which is unfortunately not written in functional English readable by laypeople).
Reverse transcription of mRNA into the DNA. This is indeed possible. Reverse transcription of covid viral RNA into DNA has been documented, Reverse-transcribed SARS-CoV-2 RNA can integrate into the genome of cultured human cells and can be expressed in patient-derived tissues (the authors theorize that this may be a reason that people continue to test positive on PCR tests months after the covid infection was resolved and cleared from the body).
The study Worse Than the Disease? Reviewing Some Possible Unintended Consequences of the mRNA Vaccines Against COVID-19 provides “a plausible scenario, supported by previously established pathways for transformation and transport of genetic material, whereby injected mRNA could ultimately be incorporated into germ cell DNA for transgenerational transmission”.
Thus it is undeniably plausible that this can happen to vaccine mRNA as well. The potential impact of this, or even the degree which this occurs, is of course also unknown due to the failure to conduct the necessary pharmacokinetic studies that could resolve such ambiguities.
Shortly after I wrote this article, a new blockbuster study came out where they documented the actual transcription of vaccine mRNA into DNA in-vitro (in a laboratory): Intracellular Reverse Transcription of Pfizer BioNTech COVID-19 mRNA Vaccine BNT162b2 In Vitro in Human Liver Cell Line. Money quote: “We also show that BNT162b2 mRNA is reverse transcribed intracellularly into DNA in as fast as 6 h upon BNT162b2 exposure.”
Although there is much more to say about all of these, this is hopefully sufficient. One final point in conclusion though: one of the more peculiar discoveries the authors of the landmark study Persistence of SARS CoV-2 S1 Protein in CD16+ Monocytes in Post-Acute Sequelae of COVID-19 (PASC) up to 15 Months Post-Infection made (although I couldn’t find the study offhand, but I heard Dr. Ram Yogandra (one of the authors) explicitly state this while being interviewed by Dr. Mobeen Sayed) was that when they sequenced spike proteins from long-covid and ‘long-vaccine’ patients, they found mutant pieces of S1 spike subunits only in vaccinated patients but not in ‘long-covid’ patients. This is very plausibly connected to the mRNA design concerns raised above. And of course, we have no idea regarding the short or long term implications of this.
Spike Protein
As everyone knows, the genetic covid vaccines encode for a modified version of the famous spike protein. Most people however - including and perhaps especially medical professionals - remain unaware that the spike protein is an incredibly toxic and biologically active protein. Thus, the specter of a broad spectrum of biological harms inflicted by circulating spike proteins is well-founded and strongly indicated.
This one salient fact is by itself sufficient to defoliate the genetic covid vaccines of their “vaccine” status. The entire point of a vaccine is to get immune exposure to the antigen/pathogen without the risks associated with infection with the live virus or disease. A vaccine that is comprised of a potently toxic and energetically bioactive protein is not a vaccine by any conventional definition.
(In fact, the study Comprehensive investigations revealed consistent pathophysiological alterations after vaccination with COVID-19 vaccines actually reported that “besides generation of neutralizing antibodies, consistent alterations in hemoglobin A1c, serum sodium and potassium levels, coagulation profiles, and renal functions in healthy volunteers after vaccination with an inactivated SARS-CoV-2 vaccine. Similar changes had also been reported in COVID-19 patients, suggesting that vaccination mimicked an infection.” Or the study “Vaccine-Induced Covid-19 Mimicry” Syndrome [etc]: - the title says it all. And the prestigious scientific publication Nature finally admitted (albeit very cautiously) on behalf of the medical establishment that long-vax is remarkably similar to long-covid in a rare critical look at vaccines: In rare cases, coronavirus vaccines may cause Long Covid–like symptoms. The upshot of all this is that the covid vaccines can cause a disease state remarkably similar to the covid disease caused by the SARS-CoV-2 virus that the these vaccines are trying to protect you from.)
How could such a consequential oversight happen? Well, when the covid vaccines were designed, we were unaware that the spike protein was the piece of covid that did most of the damage. In the intervening months after the vaccines were already in human trials, the medical literature started figuring this out, but by then it was too late to redesign the vaccines (for Pharma and government agencies that had gone all-in on the vaccine as the exit ramp from covid).
Hopefully, the readily apparent foolishness of designing a vaccine against a virus without understanding its pathology should at least be obvious going forward.
Here is a partial list of studies documenting spike protein toxicities and bioactivity:
The spike protein of SARS-CoV-2 induces endothelial inflammation through integrin α5β1 and NF-κB
The S1 protein of SARS-CoV-2 crosses the blood–brain barrier in mice
SARS-CoV-2 Spike Protein Impairs Endothelial Function via Downregulation of ACE 2
Be aware of SARS-CoV-2 spike protein: There is more than meets the eye
SARS-CoV-2 direct cardiac damage through spike-mediated cardiomyocyte fusion
Human Hematopoietic Stem, Progenitor, and Immune Cells Respond Ex Vivo to SARS-CoV-2 Spike Protein
SARS-CoV-2 spike protein-mediated cell signaling in lung vascular cells
Honorable Mention:
We still have no idea what the quantity of spike protein produced by the genetic therapy mechanism of these vaccines is, just that it can be massive. Another fun fact though: one of the modifications made to the spike proteins of the various covid vaccines was to lock the S1 into an open conformation with the RBD’s in an ‘up’ position - something virtually guaranteed to enhance the binding affinity of the spike proteins with various cellular receptor proteins.
However, it is obvious that producing billions (trillions?) of highly toxic proteins is highly problematic.
Biodistribution
Aka, where do the injected sera of and protein produced by these vaccines end up inside the human body? This is relevant because where something ends up can make all the difference in whether it will be toxic, and how toxic or what damage it is likely to be or do. There are some snake venoms that are harmless if swallowed but lethal if injected into the bloodstream. To underscore the importance of the biodistribution, one of the heroic military whistleblower physicians told Daniel Horowitz that the below cited Pfizer biodistribution study is basically a roadmap that accurately predicts the vaccine injuries that they are seeing.
Anyway, the answer to this question unfortunately is that they go pretty much… everywhere. Pfizer’s now infamous biodistribution study that was part of a pharmacokinetic package done for the Japanese government found that the LNP’s go everywhere and anywhere, with special affinity for the liver, spleen, and ovaries.
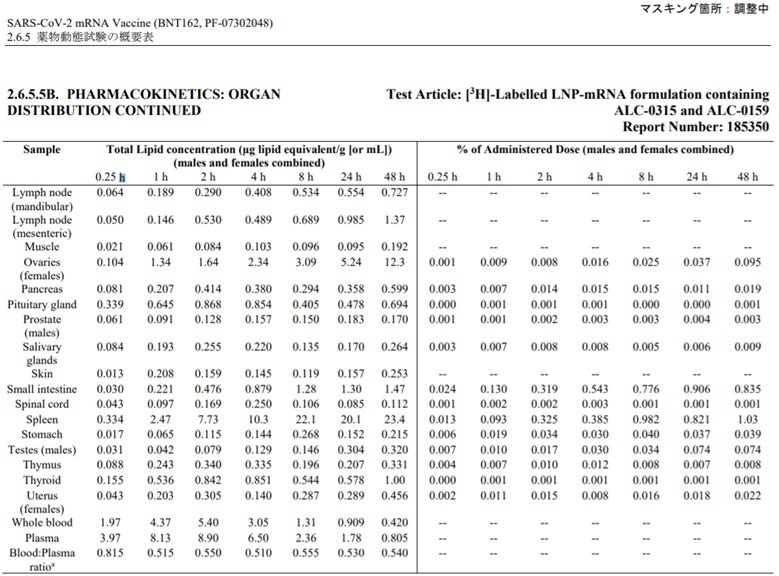
Whoops.
We also know that spike proteins themselves circulate all over, as has been documented by everyone from Harvard researchers trying to establish a control group to pathologists finding spike proteins in diseased organ tissues in autopsies.
Spike proteins have also been found in circulating exosomes (e.g. Cutting Edge: Circulating Exosomes with COVID Spike Protein Are Induced by BNT162b2 (Pfizer–BioNTech) Vaccination prior to Development of Antibodies: A Novel Mechanism for Immune Activation by mRNA Vaccines) that can be excreted through exhalation or other mechanisms, providing mechanistic plausibility for the transmission or “shedding” of spike proteins from a vaccinated individual to others.
Spike proteins likewise can end up in breast milk, similar to many other proteins circulating in the blood of the mother. (For the record, the vaccine mRNA can find its way to breastmilk as well, as is documented in the aptly titled “BNT162b2 vaccination induces SARS-CoV-2 specific antibody secretion into human milk with minimal transfer of vaccine mRNA”.)
And because spike proteins are very conspicuous in blood plasma, blood banks are likely contaminated by the bloodclot-inducing spike proteins.
How the Vaccines Engage the Immune System
Unlike previous conventional vaccines, the genetic covid vaccines markedly differ in how they engage and interact with the immune system. And of course, we have no idea what the effects of this will be (actually we have some idea now and it is rather ominous). As this spans the entirety of the immune system, it would be a hopelessly Sisyphean task to try and cover them all (and I lack the expertise to properly do so).
Autoimmune Diseases
The spike protein has epitopes (sections) that are shared with normal human proteins. Thus, some antibodies produced against the spike protein can also target and destroy normal human proteins that are quite necessary to your health.
Pathogenic antibodies induced by spike proteins of COVID-19 and SARS-CoV viruses found that,
“these pathogenic antibodies, through a mechanism of Antibody Dependent Auto-Attack (ADAA), target and bind to host vulnerable cells or tissues such as damaged lung epithelium cells, initiate a self-attack immune response, and lead to serious conditions including ARDS, cytokine release, and death. Moreover, the pathogenic antibodies also induced inflammation and hemorrhage of the kidneys, brain, and heart. Furthermore, the pathogenic antibodies can bind to unmatured fetal tissues and cause abortions, postpartum labors, still births, and neonatal deaths of pregnant mice.”
Addressing anti-syncytin antibody levels, and fertility and breastfeeding concerns, following BNT162B2 COVID-19 mRNA vaccination found a clear relative increase in what they were measuring as a proxy for anti-syncytin-1 antibodies between pre-vaccination and post-vaccination (Figure 2B). (This was a horribly confusing and incoherent mess of a study though, to be sure.)
Furthermore, antibodies the body makes to clear out the antibodies to the spike protein (yes this really does exist however weird or counterintuitive it may sound to a layperson) can bind to ACE2 receptors crucial to critical biological systems. As put by Development of ACE2 autoantibodies after SARS-CoV-2 infection:
“We hypothesized that autoantibodies against ACE2 may develop after SARS-CoV-2 infection, as anti-idiotypic antibodies to anti-spike protein antibodies. […] Many patients with a history of SARS-CoV-2 infection have antibodies specific for ACE2. Patients with ACE2 antibodies have lower activity of soluble ACE2 in plasma. Plasma from these patients also inhibits exogenous ACE2 activity. These findings are consistent with the hypothesis that ACE2 antibodies develop after SARS-CoV-2 infection and decrease ACE2 activity. This could lead to an increase in the abundance of Ang II, which causes a proinflammatory state that triggers symptoms of PASC.”
Another pathway to autoimmunity is discussed by Dr. Byram Bridle in the same report referenced above, where after a lengthy discussion of various pathways whereby the vaccines can induce autoimmunity he concludes “This is speculation but is based on a huge body of scientific literature looking at how autoimmune diseases get started. Notably, this could potentially happen in any of the tissues seeded with the vaccine if they start to express the spike protein. This is certainly worthy of investigation before the mass vaccination of children, adolescents, and young adults of childbearing age.”
There are also other mechanisms whereby a sudden and massive bolus of antibodies might be detrimental even without selective binding affinity to specific human proteins. And since this is of course unstudied in these vaccines, we are flying blind.
The lack of a complementary pathogen
Unlike other vaccines, and definitely unlike viral infection, with the genetic covid vaccines the immune system never sees an invading pathogen. Rather, it just happens across a sudden and extreme burst of spike proteins. How might this impact the training of the immune system? That’s a good question. But it is undeniable that the immune system is being “reprogrammed” by these vaccines. Exhibit A: The BNT162b2 mRNA vaccine against SARS-CoV-2 reprograms both adaptive and innate immune responses. Now, that was definitely not supposed to happen. And yes, this was not limited to the immune response to covid:
“Interestingly, however, the BNT162b2 vaccine also modulated the production of inflammatory cytokines by innate immune cells upon stimulation with both specific (SARS-CoV-2) and non-specific (viral, fungal and bacterial) stimuli.”
The study Decoding COVID-19 mRNA Vaccine Immunometabolism in Central Nervous System: human brain normal glial and glioma cells by Raman imaging similarly described their findings: “The results obtained for mitochondria, lipid droplets, cytoplasm may suggest that COVID-19 mRNA (Pfizer/BioNT) vaccine reprograms immune responses”.
Scientists should have been more deferential to the complexity of the immune system than their own God-complex. Perhaps they would then be more reluctant to believe in their own mastery and ability to selectively manipulate the immune system without any unanticipated consequences.
Influence of altered cellular biome upon the immune system
How does hijacking cells with Gerry-rigged mRNA impact the immune system? We don’t know the answer to that either, nor do we know how any of the other modified characteristics of the LNP’s or mRNA or the other ingredients in the vaccines can trigger unexpected biochemical activity (unexpected mostly by the scientists). It would have been helpful to do some pharmacokinetic testing to measure various biomarkers that could at least produce a grainy picture, but the FDA elected not to require that. We do have synthetically boosted immunologically invisible mRNA due to ‘modifications’ like the m1Ψ though.
mRNA or spike protein taken up in phagocytic cells
Phagocytes are immune cells that are sort of akin to Pacman, gobbling up viral particles (and other stuff that doesn’t belong). As stated earlier, we now know that spike proteins are persisting in different phagocytes, notably certain types of monocytes, sometimes indefinitely. It is possible that LNP’s with mRNA are also penetrating or getting swallowed by immune cells. We don’t know what is necessarily causing this, and we certainly don’t know what the impacts of this might be. We do know that certain monocytes seem to be ‘activated’ by having pesky spike proteins inside to spew the highly inflammatory cytokines everywhere, which is of course not exactly a positive development.
LNP’s as an adjuvant
The covid vaccines seem to rely upon the LNP’s to serve as the vaccine’s adjuvant, as they are very pro-inflammatory on their own (an adjuvant is something designed to provoke the immune system to respond to the antigen or antigenic proteins in a vaccine). Needless to say, we don’t know what a massive infusion of highly provocative pro-inflammatory LNP’s going everywhere in the body does to the immune system’s massively complex network of various types of cells or how it may ‘miseducate’ the immune system in detrimental ways, as indicated above.
The effects of everything else mentioned above on the immune system
Any of the numerous mechanistic pathways of pathogenicity enumerated to this point can easily engage the immune system in unhealthy ways. There certainly is some degree of serious immune suppression going on in a significant number of people, so much so that there is now talk of “Vaccine AIDS”. The veritable explosion of cancer diagnosis and sudden and rapid metastasis of cancers in remission or under control ominously portends a cancer tsunami that may well end many more lives than covid did.
Vaccine Manufacturing & Administration
Manufacturing complex biologic therapeutics is an extraordinarily sophisticated and delicate process that requires a ton of specialized expertise by many of the personnel involved in the manufacturing process. It is therefore highly regulated by the FDA (and other medical regulatory agencies around the world), because even a small hiccup or mistake can contaminate or ruin the final product.
So has has the manufacturing of the covid vaccines been going so far? Let’s take a look:
Manufacturing Snafus
Consider the following events:
How did 75M J&J vaccines get ruined? FDA details the manufacturing woes at Emergent's beleaguered site. The FDA subsequently issued a report, FDA review memorandum 06112021.
Stainless Steel Contamination: Japan: 1.6m Moderna vaccines recalled; Novavax replacement deal signed / Japan halts use of 1.63 mil. Moderna vaccine doses over contamination
Pfizer facing 'various challenges' in COVID-19 vaccine manufacturing, dosing: feds
Pfizer’s Newest Vaccine Plant Has Persistent Mold Issues and a History of Recalls.
Did they adequately fix any of these issues? Were these issues problematic elsewhere but went undiscovered? Of course, the companies and individuals involved (implicated?) say that they fixed the problems and that any issues were limited to where they got busted, but that isn’t exactly evidence. Considering that there seem to be recurring or persistent manufacturing issues everywhere, there is reason to suspect that the cut corners may encompass the manufacturing processes too in addition to the clinical testing.
There is enough here to worry that there might be quality control issues with the unprecedented sudden and rapid scaling up of manufacturing capacity of a novel biologics product.
Real-world results seem to bear out this concern. The British Medical Journal documented a very significant range of inconsistency between different vaccine batches: BMJ: Leaked documents show that some early commercial batches of Pfizer-BioNTech’s covid-19 vaccine had lower than expected levels of intact mRNA - The EMA covid-19 data leak, and what it tells us about mRNA instability | The BMJ. A few of the biggest chemists in Germany penned a letter to the CEO of Pfizer’s partner BioNTech, German Chemists Write Letter to BioNTech Asking About ‘Impurities’ Causing Pfizer Vax to Turn a Concerning ‘Shade of Gray’. (Although BioNTech issued a response dismissing their concerns, we do not resolve investigations through press releases by parties with a vested interest in the outcome.)
Regarding the AstraZeneca vaccine, the study Process-related impurities in the ChAdOx1 nCov-19 vaccine reports that “the vaccine, in addition to the adenovirus vector, contains substantial amounts of both human and non-structural viral proteins. Among the human proteins, heat-shock proteins and cytoskeletal proteins were particularly abundant. The often-observed strong clinical reaction one or two days after vaccination is likely associated with the detected protein impurities. A linkage to later immune-related adverse events is also conceivable.” Where were the regulators? Apparently not bothered enough to look into this. The authors go on to suggest (observe really) that the “identification of specific classes of protein impurities should guide and accelerate efforts to increase the purity of the vaccine and increase its safety and efficacy.”
And it’s not like manufacturing inconsistency is a new issue - New Quality-Control Investigations on Vaccines: Micro- and Nanocontamination documents what its title suggests. The measurement and full statistical analysis including Bayesian methods of the aluminium content of infant vaccines discovered that out of the thirteen infant vaccines they tested, “only three vaccines contained the amount of aluminium indicated by the manufacturer. Six vaccines contained a statistically significant (P < 0.05) greater quantity while four vaccines contained a statistically significant (P < 0.05) lower quantity. The range of content for any single vaccine varied considerably, for example, from 0.172 to 0.602 mg/vaccine for Havrix”.
Storage Requirements
The covid vaccines need to be stored at extremely cold temperatures in order to preserve the integrity of the mRNA (and some of the other components or chemistry as well). There is no basis to assume that the storage requirements have been religiously followed. The way we would typically keep track of this sort of thing is by random testing of batches at various points in transport, storage, and thawing, which of course isn’t being done. And even if regulators wanted to do testing, it is unclear if they could do so effectively at this point, because the FDA skipped requiring the vaccine makers to do a full workup of what the chemical state of the vaccines would be at various temperatures, for various amounts of time, and so on. In other words, we don’t even have a clear baseline to test against to see if the vaccine in the vials looks like there was a failure to maintain the prescribed storage parameters.
And what happens if we use degraded mRNA not kept adequately frozen? Good question. For instance, we have no idea what the results of translating degraded sections of the mRNA might be.
Vaccine Administration
Last but not least, there is good old fashioned human error. Injecting the vaccine isn’t quite as simple as sticking the needle in someone’s arm and depressing the plunger. As the CDC guide COVID-19 Vaccine Administration Errors Revaccination Guidance documents, there are a whole assortment of possible mistakes one can make.
And make them they have (which is hardly surprising when you consider that the people hired are not exactly top-of-the-line nurse practitioners or health care professionals). There have been a bevy of reported adventures in vaccine misadministration, such as “Nearly 4,000 Kaiser patients may have received wrong COVID vaccine dosage in Bay Area” or “Bay Area Sutter Health clinic gives 14 kids wrong COVID vaccine dose”. Project Veritas released a stunning video documenting some shocking bombshells where employees were not following the proper directions for the preparation and administration of the covid vaccines (and this was for children).
Finally, multiple studies (e.g. Intravenous injection of COVID-19 mRNA vaccine can induce acute myopericarditis in mouse model; or Thrombocytopenia and splenic platelet directed immune responses after intravenous ChAdOx1 nCov-19 administration) have suggested that the risk of myocarditis is significantly higher where the vaccine is injected (accidentally) directly into a blood vessel. The authors of the first study conclude “This study provided in-vivo evidence that inadvertent intravenous injection of COVID-19 mRNA-vaccines may induce myopericarditis. Brief withdrawal of syringe plunger to exclude blood aspiration may be one possible way to reduce such risk.” A Rapid Response to SARS-CoV-2 vaccination and myocarditis or myopericarditis: population based cohort study published in the BMJ similarly suggested that “a significant factor increasing the risk of myocarditis or myopericaditis is the current mode and procedure by which these mRNA vaccines are administered to patients. […] If aspiration is not carried out first before injection, there is no means to check whether accidental injection into a blood vessel has occurred.”
The risk of other vaccine-associated injuries might also be elevated if the vaccine is injected intravenously. Cerebral venous thrombosis after COVID-19 vaccination: is the risk of thrombosis increased by intravascular application of the vaccine? concluded exactly what its title suggests.
Lastly, like all the other potential adverse pathological mechanisms of the genetic covid vaccines, we have no idea what else might depend on the injection route.
As has been demonstrated, there are numerous legitimate concerns with the genetic covid vaccines. Yet the basis for all of the claims of vaccine safety ultimately are merely expert opinion (and from incredibly subpar experts to boot). Expert opinion does not constitute clinical evidence, and is certainly not a viable standard to adjudicate the safety profile of novel therapeutics. Were expert opinion a valid method of adjudicating safety concerns for new medical products, the FDA could be retired, as the experts almost always assume new drugs won’t have any unanticipated side effects. Just compare the original claims that “it is scientifically impossible for the vaccines to have safety issues” and “it’s not plausible that ______” to what has been articulated above. What a rational person would take away from this is that the medical community is filled with infantile idiots who are functionally illiterate in the very subjects they profess to be experts in (and that is from a merely superficial and cursory overview of the real medical science).
Regrettably, experts seldom recognize the limits of their own expertise, and vis a vis covid seem unaware that any exist altogether. Thus we should be especially wary that we are indeed adhering to the foundational ethic of medicine: “First, do no harm.”
If anyone notices anything I missed, or stated inaccurately, please feel free to leave a comment.
The most comprehensive summary so far. Thank you!
include also our paper on codon optimization https://www.mdpi.com/1422-0067/22/12/6490
original spike has pausing site optimized versions do not have.