The goal of this article is to demonstrate that the following two propositions are strongly indicated by the death certificate data from Vermont:
The covid vaccines did not at any point demonstrate discernable efficacy against severe covid disease or death.
The most straightforward plausible interpretation of the data is that the covid vaccines caused covid disease to become markedly more severe.
The crux of the argument for of these propositions is that covid disease-related deaths substantially increased following mass vaccination with the covid vaccines in Vermont, where population that suffered the vast majority of such deaths occurred had a >95% vaccination rate. This is not something that can be plausibly or realistically explained if the vaccines provided any degree of meaningful protection against covid disease morbidity/mortality.
It is worthwhile to demonstrate both of these propositions, because they are separate and distinct destructive consequences of the mass vaccination campaign, each with unique ethical considerations. Importantly, if the 2nd proposition is true, it would be unethical to allow the population at large to make an individual choice to get vaccinated, because of this negative externality elevating the risks faced by everyone else from a more virulent and lethal viral pathogen.
How can we distinguish legitimate covid disease-related deaths?
This is not a simple task. To simply tally the death certificates that mention covid is unreliable because of the absurd standards promulgated by the CDC regarding assigning covid as a CoD. Furthermore, the various tests mass deployed to test for the presence of the SARS-CoV-2 pathogen suffer from any number of varying defects that can lead to both false positives and negatives, yet anyone who died within 30 days of a positive covid test could be documented as a covid death.
Thus we must define what a covid death is, and something to measure it by.
What is a covid death?
For our purposes, we are looking for deaths that are caused - at least in part - by a pathology initiated by the covid virus and that would not have otherwise occurred in the absence of covid. The reason for the latter condition is that for deaths already baked into the cake so to speak, it makes no difference which is the precipitating pathogen or cause is, for instance a certain number of people will fall to contagious respiratory pathogens every year regardless. From a public policy perspective it is therefore irrelevant which virus happens to be the one to do the deed. What we do care about is excess deaths caused by covid that would not have happened but for the covid infection/disease - here the identity of the offending pathogen is relevant, because the other circulating common respiratory pathogens would not have otherwise killed these people.
Since this is a respiratory infection, much of the primary covid pathologies are conditions of or related to the respiratory system. So although there are other associated non-respiratory pathologies (most notably coagulopathies, but there are plenty of others), the most accurate available proxy for covid disease-related deaths should be deaths involving the associated respiratory conditions that typically occur in patients suffering severe covid disease., which should be more unique to covid compared to conditions caused by vaccine SAE’s or health problems caused by or the consequence of pandemic policies.
The following are the CoD conditions that I distilled from the CoD’s provided on the spreadsheet obtained from the state of Vermont (it would take a full article to document the numerous steps taken to curate this list, suffice it to say that it was not a simple task to sort through hundreds of potentially relevant conditions & standardize them into a condensed handful of searchable text strings).
(I am not going to use all of them in this article though.)
In a nutshell, when there is covid disease causing deaths, we should see this manifest as increases in deaths related to the potpourri of respiratory system conditions that are the manifestation of the damage caused by covid disease.
What does the data show?
*************
**NOTE: Make sure to read the labels and numbers on the charts, there are many charts that look deceptively similar that do not contain identical information.
In particular, some charts are the full calendar year, and others are only through 9/30 for each year, in order to equalize 2022 to the other years because the 2022 data we have only goes through most of October. In full calendar year charts, 2022 data runs through the first half of October.**
*************
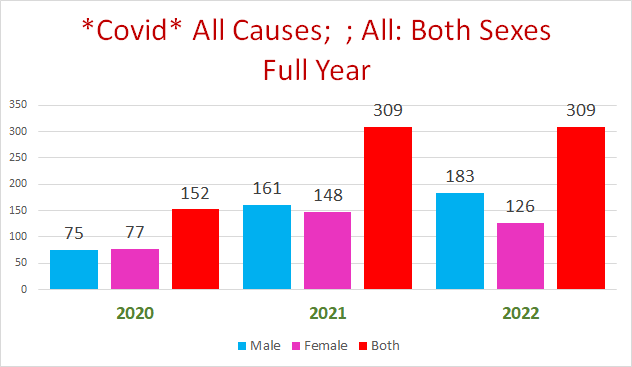
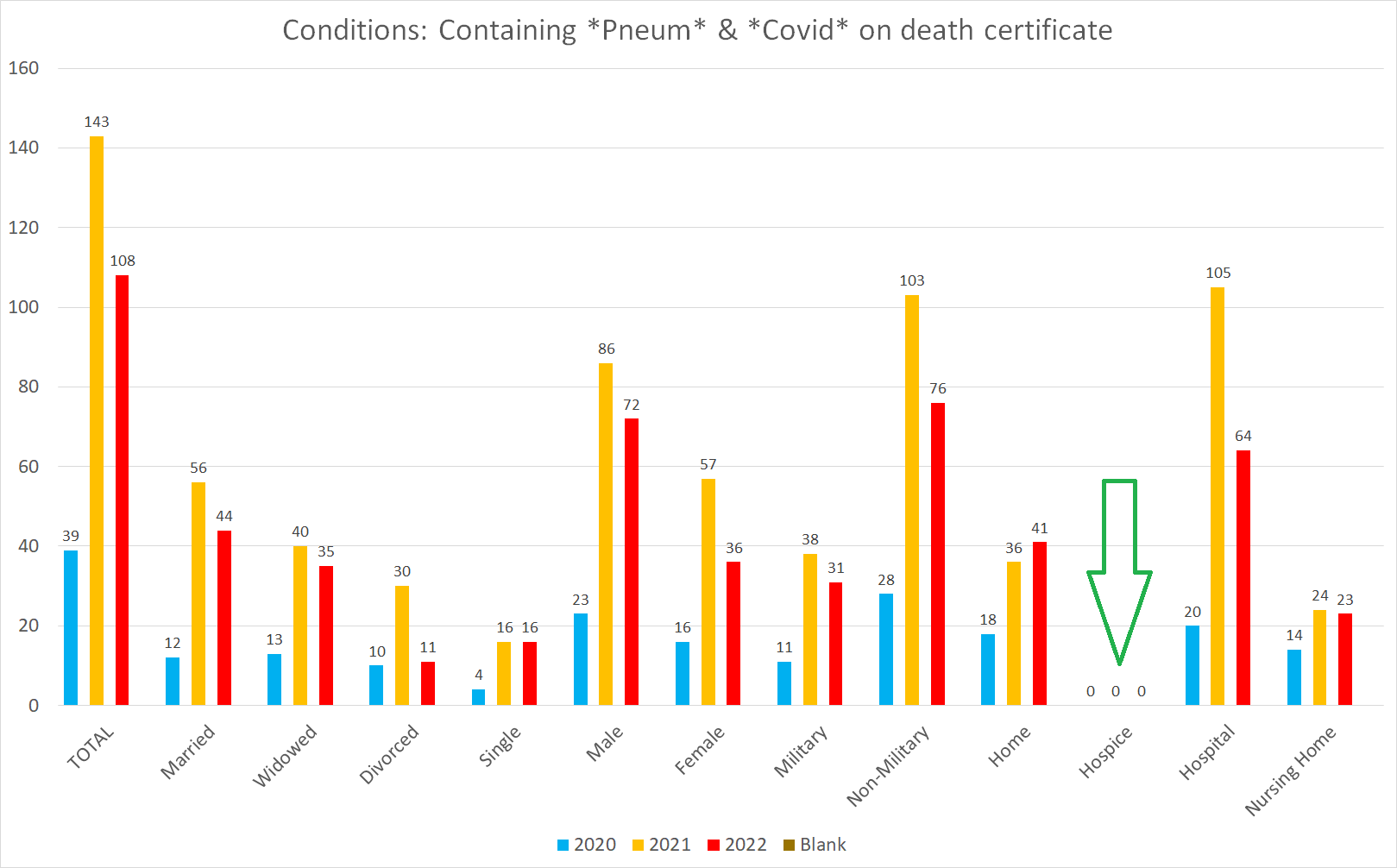
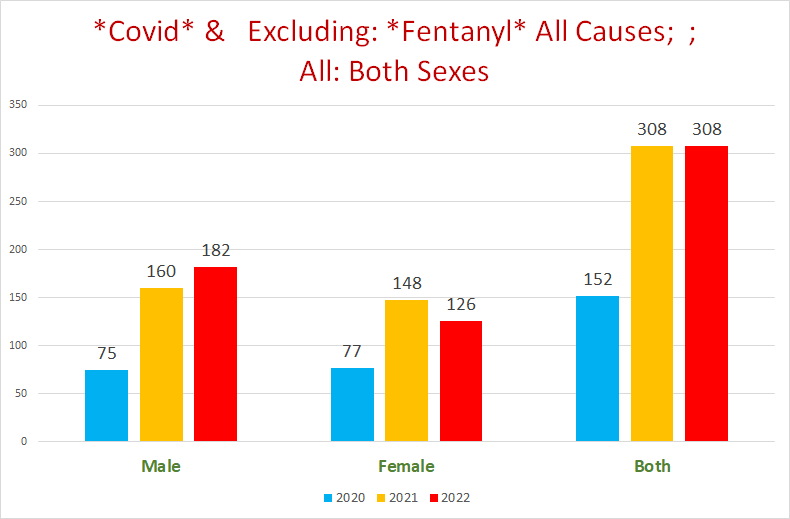
It is prudent to highlight by way of introduction that even if you look at the topline number of official covid deaths, both 2021 & 2022more than double the covid deaths of 2020; and the 2022 number is only through most of October, meaning that it will definitely be markedly higher by year’s end:
Respiratory Deaths
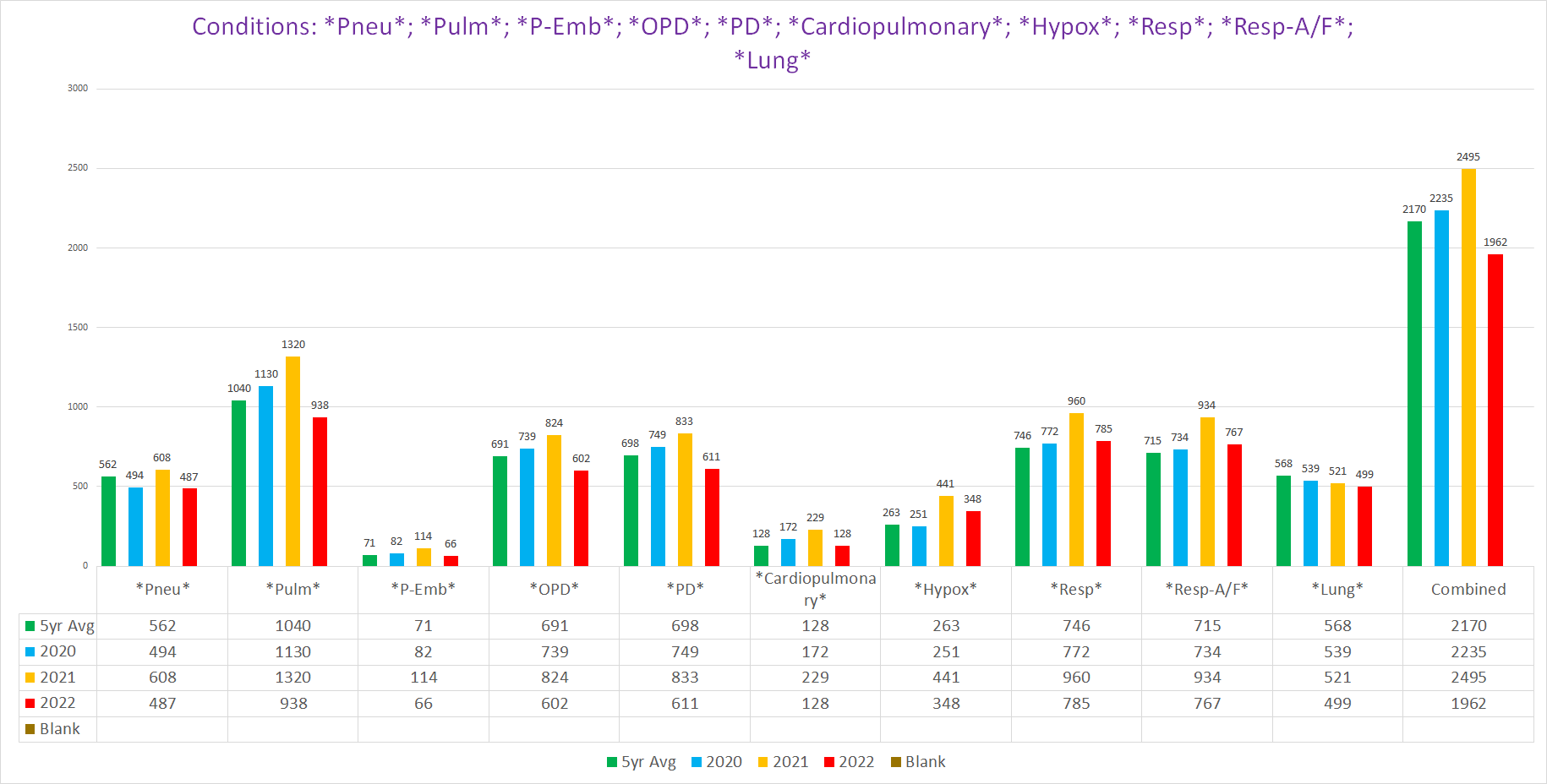
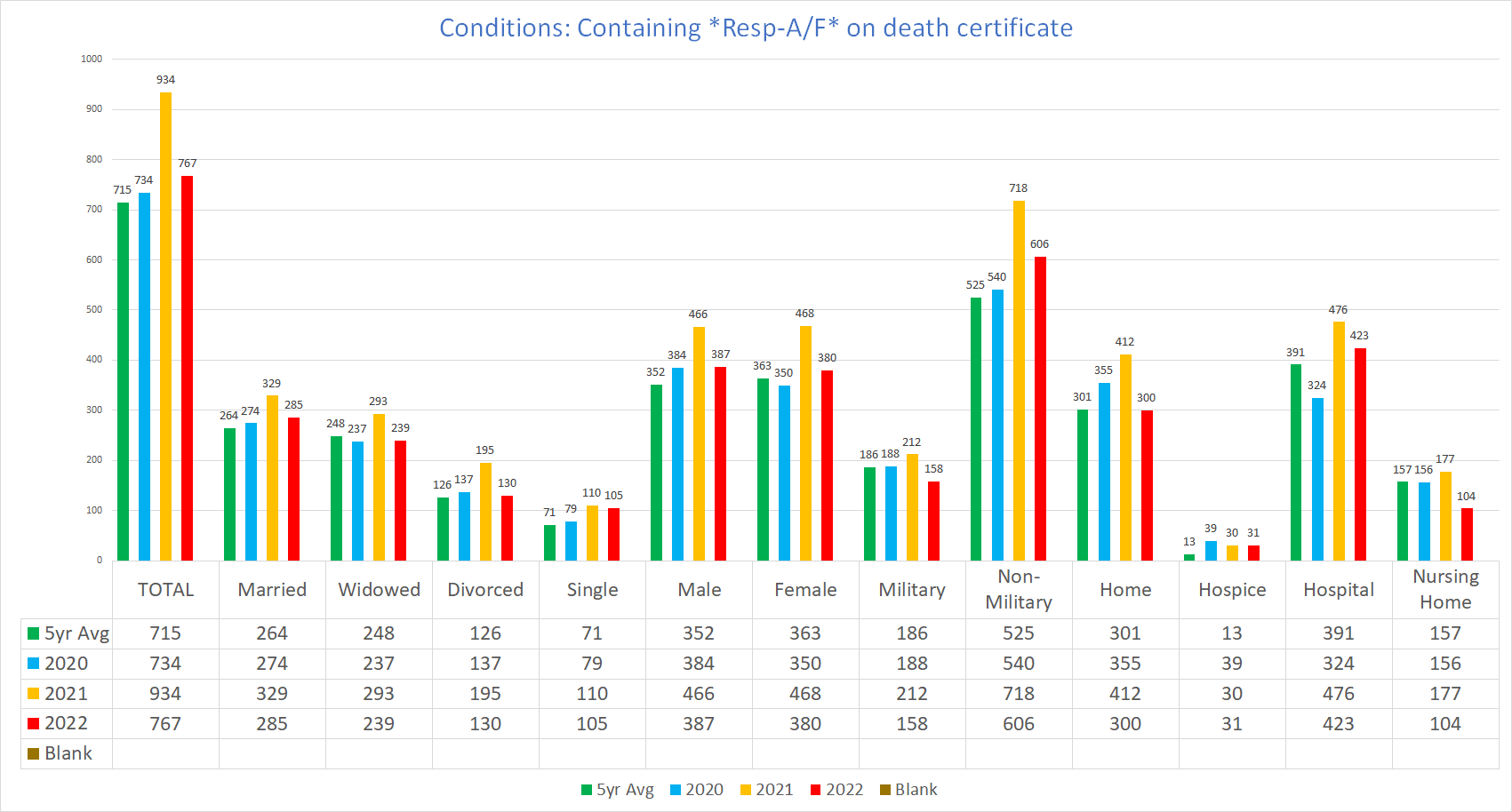
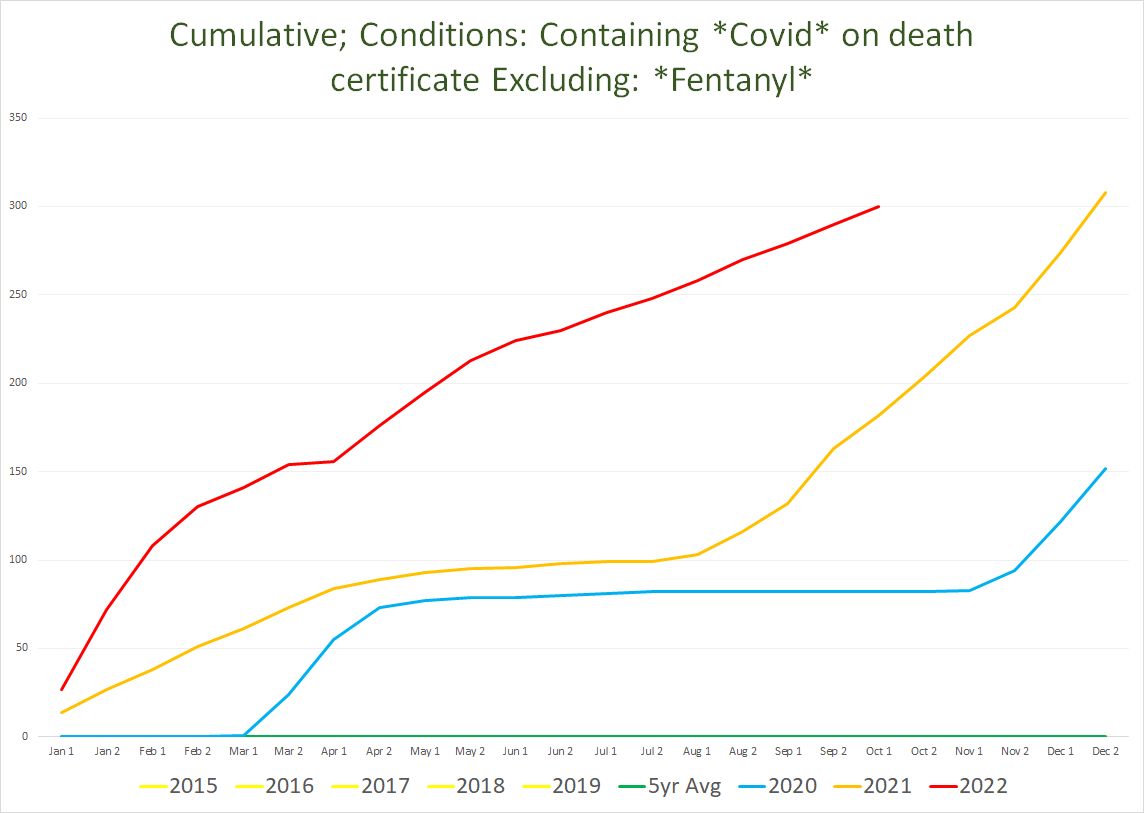
The following two charts show the various concatenated categories of respiratory system conditions for the entire calendar year, and through 9/30:
Note: the 2022 total includes those available from October on this chart but is not included in the following chart.
As you can see, 2021 dominates 2020; and 2022 is handily beating 2021 through the end of September - this despite the fact that 2022 has so far been dominated by the much milder Omicron variants.
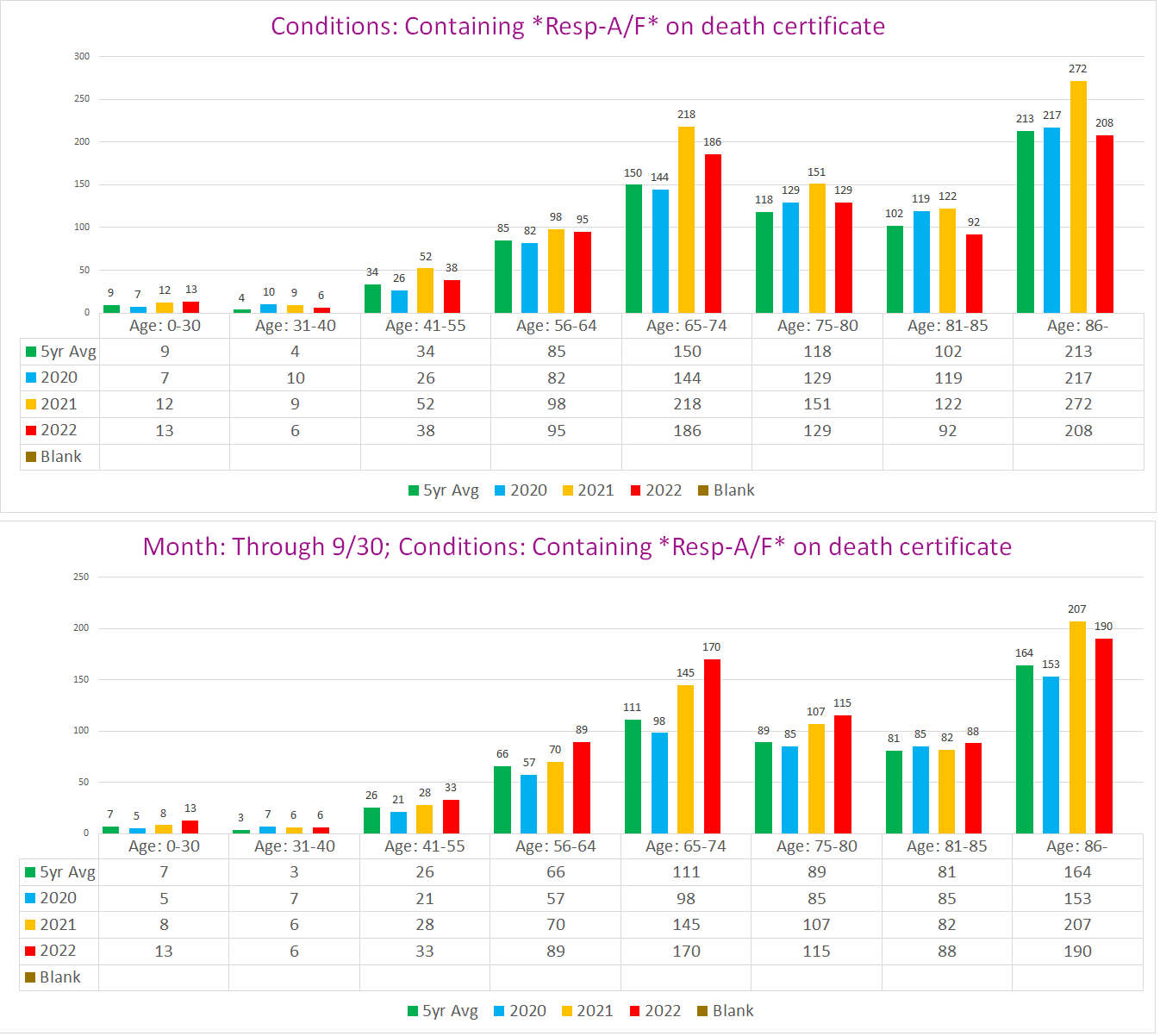
Here’s the kicker though: 2021 did not start pulling away from 2020 or the prior 5yr average until the beginning of September, when it abruptly diverges (black line):
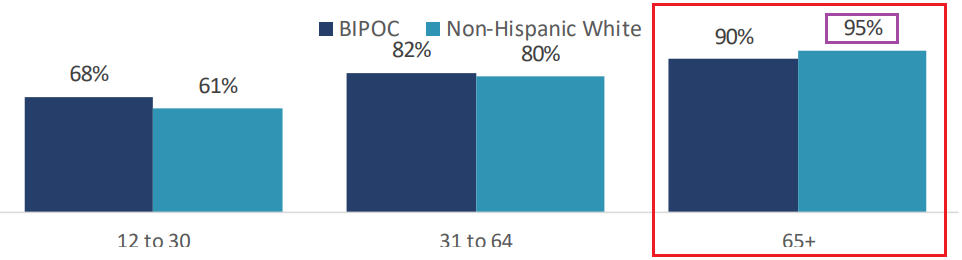
This is after Vermont had achieved 95% vaccination in non “BIPOC” seniors 65+ by September 2021 (the population of Vermont is 93.6% White according to Google); and >80% vaccination in the 31-64 cohorts:
These would be the same cohorts that suffered 98% of the additional deaths above in 2021 above 2020:
(Refer to the above list of respiratory conditions for the abbreviations)
From the combined overall total, it would seem that the real pandemic of respiratory deaths began around September 2021, well after the state was the foremost vaccine haven of US.
However, this combination of conditions might be misleading, because a few of these conditions can also be caused by vaccine adverse events unrelated to a covid or respiratory infection. We’re trying to find the covid deaths, not the vaccine SAE deaths. In order to account for this (and also other potentially interfering factors), we can look at some of these conditions individually.
It is critical to note a very profound limitation of individual condition data from these death certificates:
They are subject to the very subjective and often incompetent mercies of whomever is filling them out - meaning there can be a significant error rate contaminating the data. Additionally, circumstances can play a significant role in whether a condition gets noticed and documented, for instance deaths occurring in hospitals vs hospices might
The sample size for many conditions is too small to be reliably generalizable.
Other Notes:
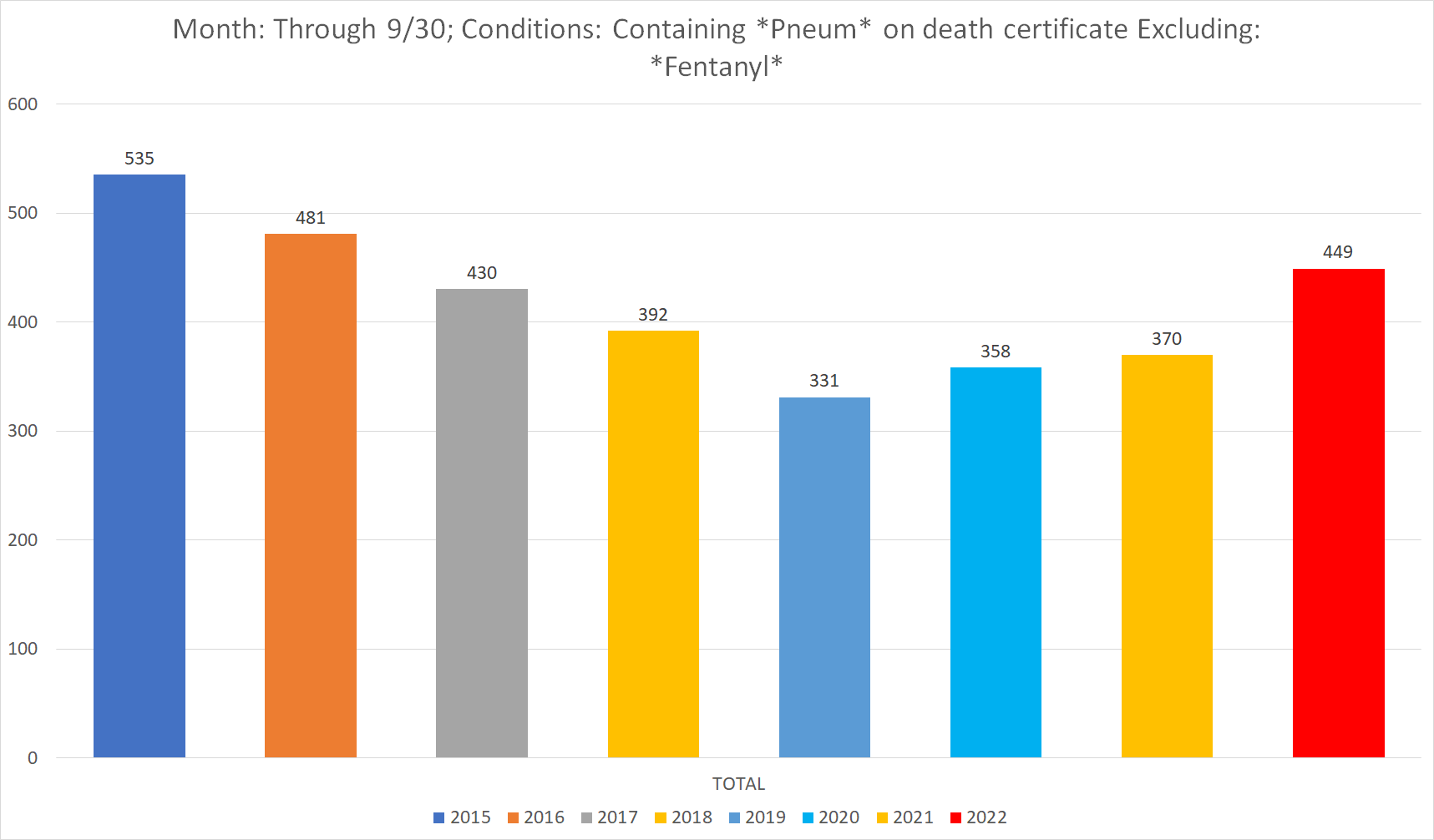
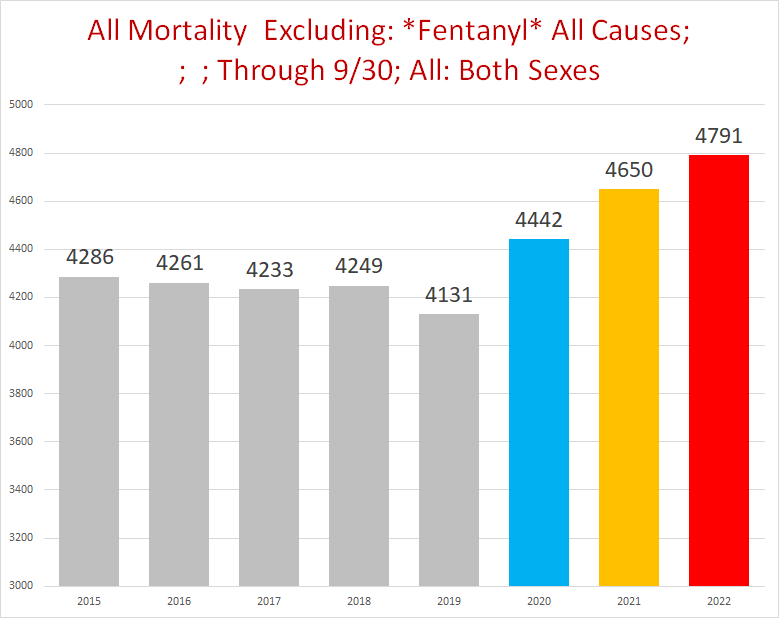
I am going to exclude any death certificate that includes Fentanyl as a CoD (which includes a solitary covid-fentanyl death)
Respiratory Arrest/Failure/Distress
I am grouping these together because they seem to be essentially the same thing - a cessation of the respiratory system to respirate that leads to death - what you’d expect to occur in a decent percentage of fatal respiratory system disease conditions. On the flip side I suspect that these are used interchangeably by ME’s.
Boy is there a signal here - 2021 really explodes out from 2020, almost like the central tower of Burj Kalifa stretching up beyond the spiral:
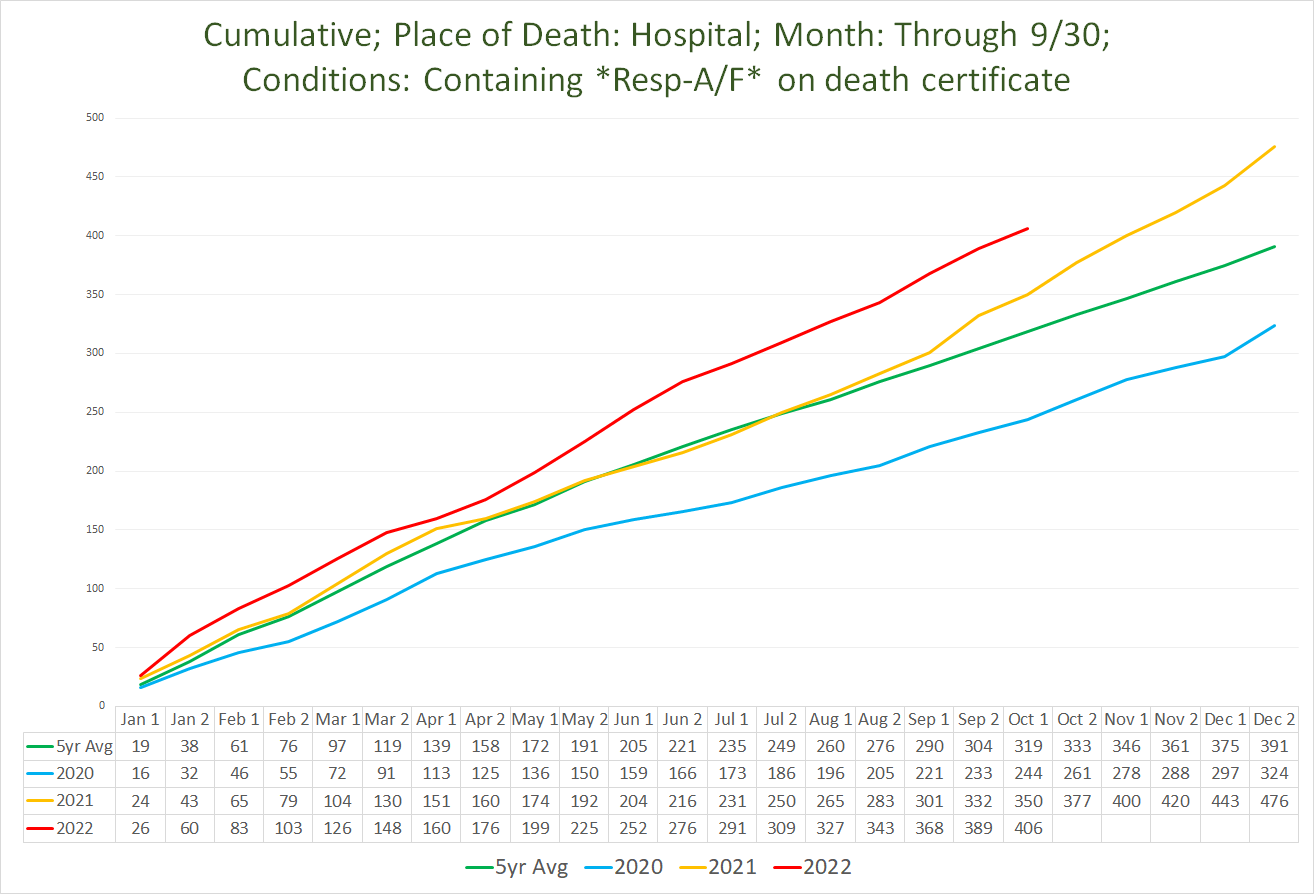
But wait! If you think 2021 was a horror show, get a load of 2022 (through 9/30 each year):
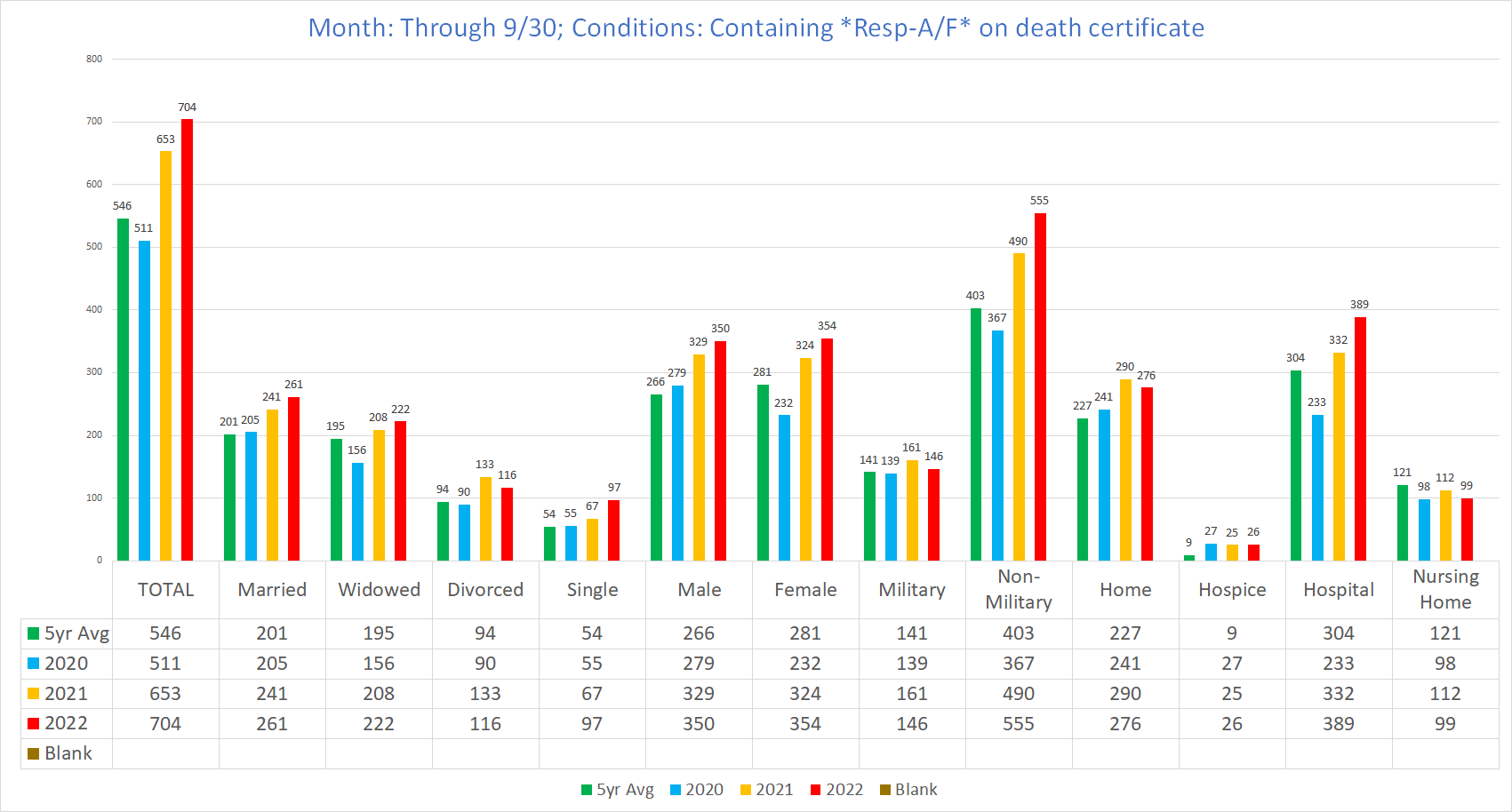
By age - full calendar year (top); through 9/30 (bottom):
Trendline:
Here we can see a more consistently elevated 2021 mortality trend above 2020 & the pre-pandemic 5yr average.
2022’s domination above even 2021 is all the more startling, as 2022 bursts out of the gate with a mortality advantage, despite Omicron already being the predominant variant. Vermont’s combination of almost full vaccination and obvious trend of increasing deaths by respiratory failure despite the marked attenuation of covid’s pathogenicity would seem to be some type/s of vaccine incited immunological suppression (whether is be V-AIDS, ADE, Original Antigenic Sin / pathological priming, immunological exhaustion, or another form of iatrogenic confounding of the immune system).
Additional Observations for Respiratory Failures:
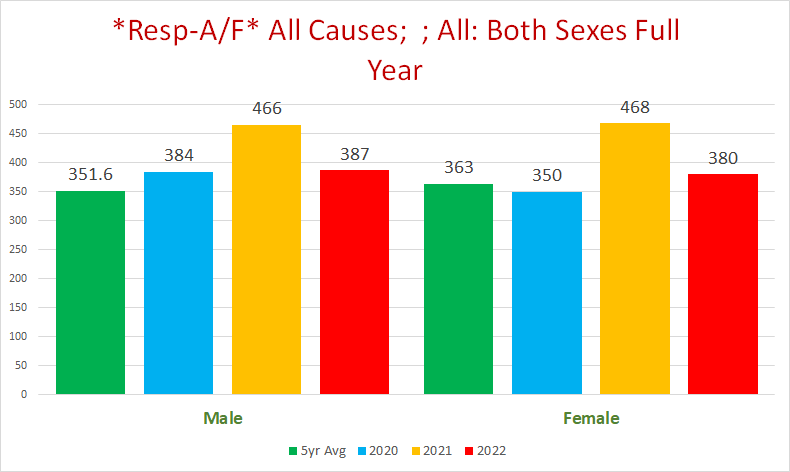
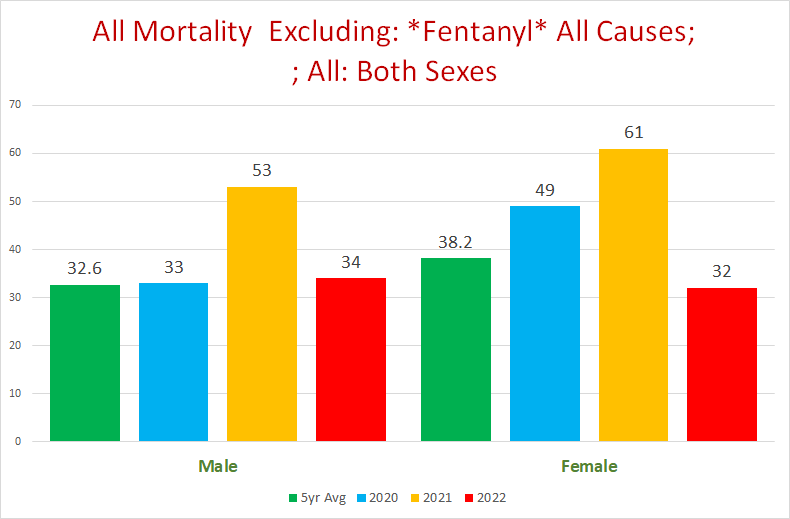
Covid was exclusively a male scourge in 2020 in Vermont
Not only did the women escape excess deaths from respiratory failure, they had a deficit compared to the 5yr pre-pandemic average, as opposed to the men who had 9.1% excess mortality from respiratory failure over the 5yr pre-pandemic average:
The excess mortality in 2022 is likely more than what the topline number suggests
2021 should result in a “pull forward” effect, so that there would be less expected deaths from respiratory failures in 2022 and the next few years than we would’ve expected without the pandemic happening, because a decent % of the excess deaths were people who were “supposed” to die in 2022 and the next few years. The fact that not only did 2022 beat the prior baseline, not only beat 2020, but also is convincingly edging out 2021 despite this is remarkable to say the least.
Hospital Statistics
Interestingly, we can see that the 2021 September surge in all respiratory conditions that continues through 2022 is perfectly reflected in the respiratory failure hospital deaths. This is quite a reversal from the substantial deficit in hospital deaths from respiratory failure in 2020, when a bunch of people died at home instead of going to the hospital (our esteemed public health experts in action).
Excess respiratory failure deaths from September 2021 onwards seem to possibly be a function of disease conditions that led to the hospitalization - or disease conditions that are introduced via hospitals (nosocomial/iatrogenic):
Once we’re on the topic of hospitals, I thought it might be interesting to see how much of an overlap there is between respiratory and renal failure/disease:
“Alexa, what are the side effects of Remdesivir?”
This will hopefully be a topic for a future article.
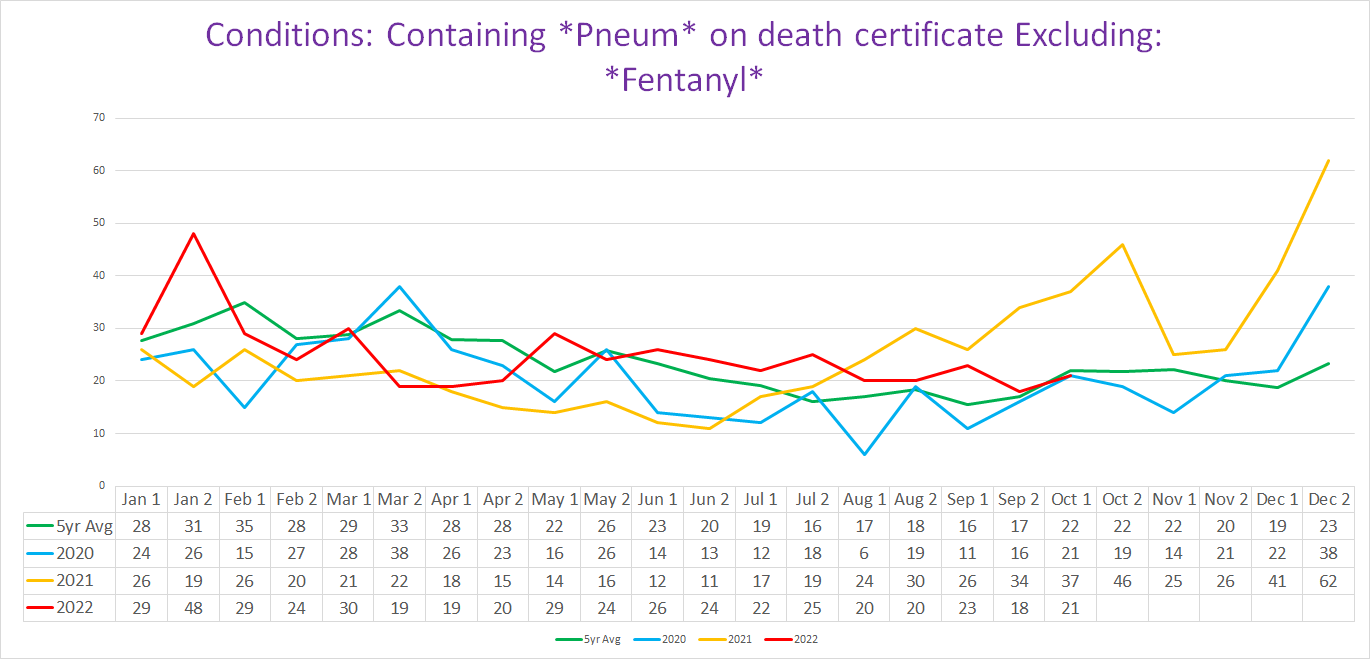
Pneumonia/Pneumonitis
If there is one disease condition that is paradigmatic for respiratory disease mortality, it is pneumonia. This is especially true for covid, which has a distinct type of pneumonia referred to as an “organizing pneumonia”, in addition to the typical bacterial pneumonias caused by opportunistic bacteria taking advantage of the patient’s severely weakened and compromised diseased state.
However, the pneumonia data is chaotic to say the least, which makes it difficult to parse out.
Here is pneumonia for the pandemic years & pre-pandemic 5yr avg:
The first thing that jumped out to me is that the 5yr average crushes 2020 big time. However, this is merely the pre-pandemic downward trend raising the average:
The overall trend is remarkably stable from 2015-2019, but is reversed in 2020, and annihilated in 2021.
If we look at the first 9 months of the year, we can see that 2022 is blowing out even 2021 to date. (The reason that the difference between 2021 and 2020 disappears is that the excess of 2021 happened almost entirely during the last three months.)
It is important to acknowledge that the pre-pandemic downward trend in pneumonias could be due at least in part to other factors besides fewer people dying, such as shifting patterns of how ME’s were coding deaths - there was definitely not a downward trend in all cause mortality:
In other words, it could be that the decreasing number of pneumonia deaths from 2016-2019 (per the downward trend) did not represent less people dying; rather the people “saved” from pneumonia were either dying but being attributed to a different CoD; or they were being replaced by other people dying instead of them, perhaps at least in part by increasing Fentanyl deaths:
(NOTE: pay attention to the Y-Axis numbers, they are NOT the same from chart to chart.)
Covid + Pneumonia: Smoking Gun?
Returning to pneumonia, although the overall trend is inconclusive, there is a specific subset of pneumonia deaths that we could use as a proxy for covid deaths: deaths with both covid *and* pneumonia. This is likely to be a decent proxy for genuine covid deaths, at least in the sense that covid really did kill most if not all of these people.
There is most definitely a whopper of a signal here - the trendline for covid + pneumonia deaths is probably the single most potent chart in this article:
This is even worse than it seems at first glance (which is itself pretty horrid). Covid + pneumonia deaths in 2022 are crushing 2021 in raw numbers, despite the fact that 2022 is dominated by the far milder Omicron variants compared to 2021 which was dominated by the brutal Delta variant; and despite what should be a pretty substantial pull-forward effect from 2021 deaths (and a little bit from 2020 too).
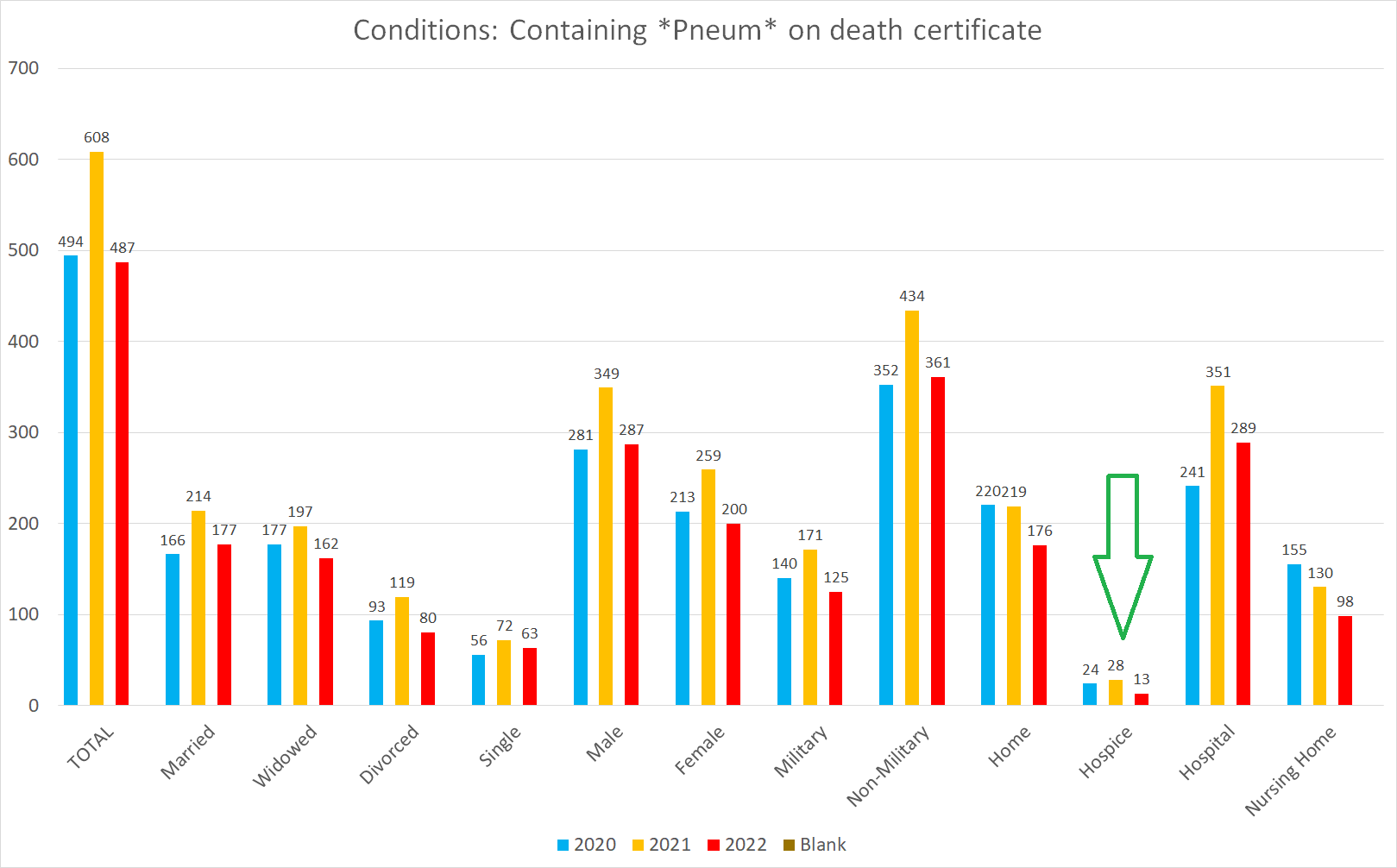
Another indicator that this combination is a fairly reliable proxy for genuine covid deaths is that there is not a single hospice death with both covid and pneumonia on the death certificate, even though there are a bunch of hospice pneumonia deaths without covid:
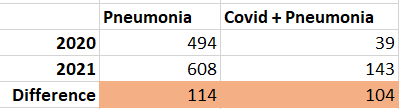
Furthermore, the difference between 2020 pneumonia deaths and 2021 pneumonia deaths is almost entirely from the increase in covid + pneumonia deaths:
This suggests that the increase in pneumonia deaths in 2021 over 2020 is attributable to covid. Covid that started ravaging the population after vaccination started, and the majority of the deaths occurred after almost the entire population was vaccinated.
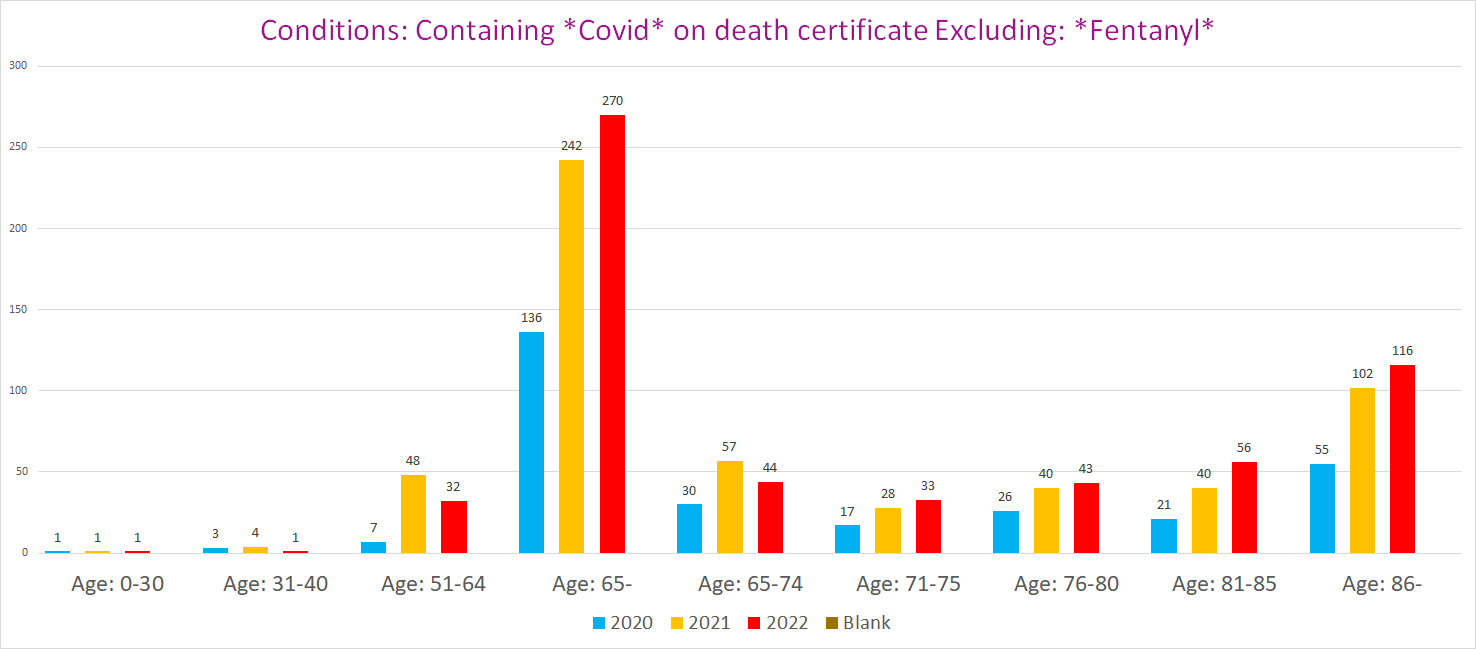
Another damning observation with the covid + pneumonia deaths is that when we break it out by age, we see the following:
There are literally 8x as many covid + pneumonia deaths for the age cohorts 41-69 in 2021 as there were in 2020.
It must be stated that it is not true that every covid + pneumonia death is by definition an excess death, because even if someone died from covid, it could be that they were one of the people who were “supposed” to die from respiratory pathogens, which in 2021 was still dominated by covid.
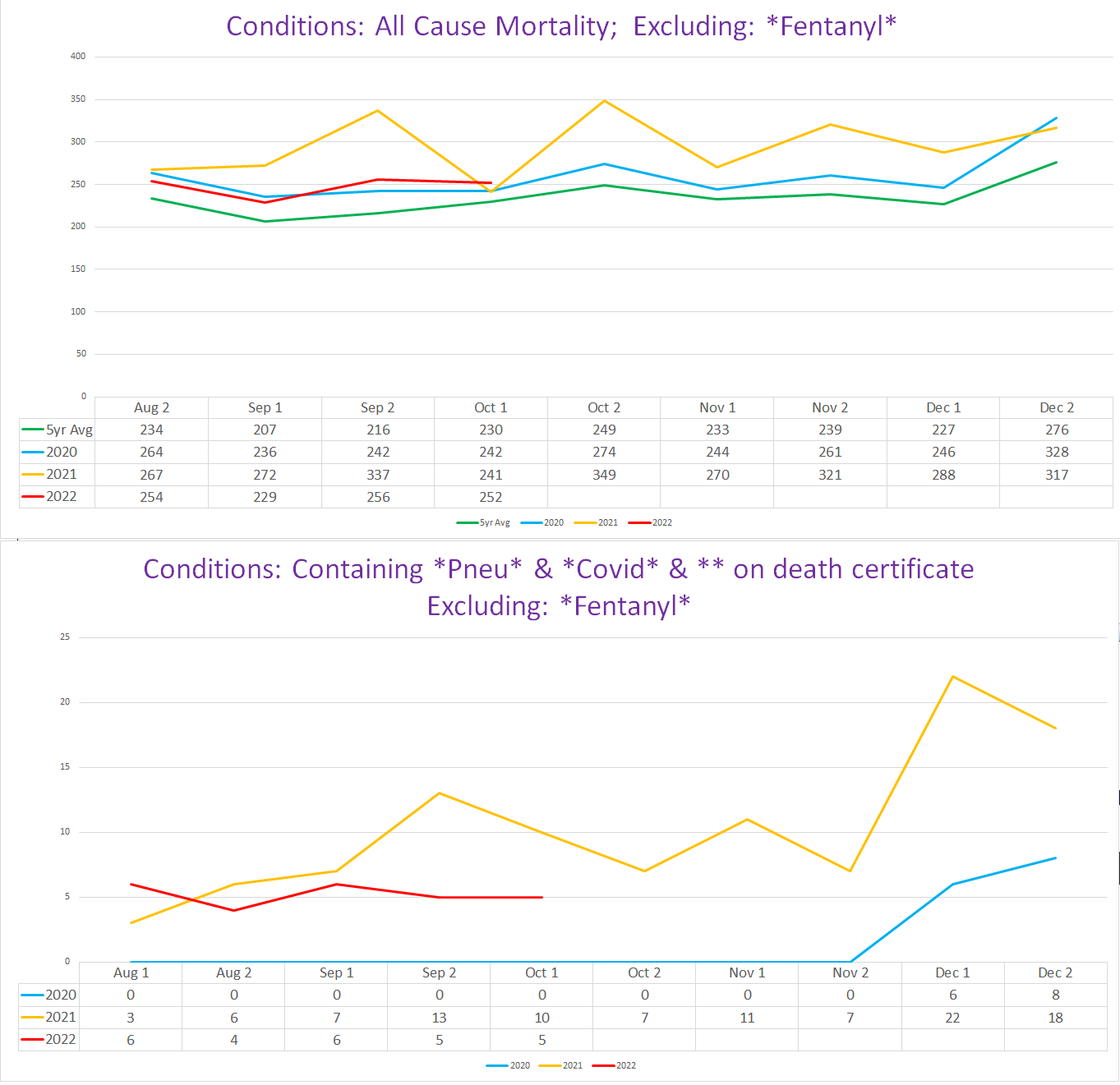
However, the fact that the glut of pneumonia + covid deaths occurs at the same time there is an upswing in excess mortality [over the pre-pandemic 5yr average] indicates that a substantial portion of these deaths (if not the vast majority) represent deaths that would not have happened but for covid:
For the record, the 5yr all-cause mortality average for 2015-2019 is pretty accurately representative of these years, especially the last 5 months which is where we see 2021 excess mortality really separate itself from prior years:
Pulmonary Emboli
Pulmonary emboli are confusing. On the one hand, PE’s are perhaps the most paradigmatic pathological complication of covid disease. On the other hand, PE’s simply do not track well with covid (although it must be stressed that VT is a small sample and there is always the possibility of randomness or some other variable that mucked things up).
Pulmonary Emboli - 2020
I covered the disconnect between PE’s and covid for 2020 previously:
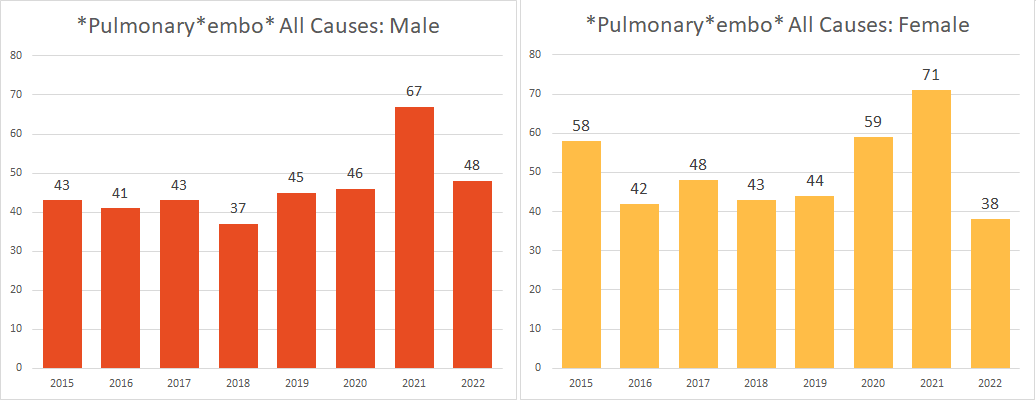
Pulmonary embolism is one of the most common covid disease complications. This was especially true for the native Wuhan strain that kicked off the pandemic. Yet there is no excess PE’s whatsoever for the men who definitely suffered a bit of excess mortality from covid, while there is definitely excess PE’s for the ladies.
If we look at when the bulk of the female excess PE’s occurred, it doesn’t seem to be covid per se either:
The excess is almost entirely from the red boxes. The first two were before covid officially swept in, the spike in September - 5+ above the 5yr avg - does not correspond to any other conceivable covid manifestation (and it would have to be a huge covid wave to cause PE’s to almost triple), and the mild November excess is similarly before the winter covid wave sets in for Vermont. Finally, when we overlay PE’s with covid, this is what we get:
Considering that anyone who died with a positive test would get covid on their death certificate - and surely so if they went on to die at least in part because of the prototypical complication of covid disease - the stark dissociation of PE’s and covid seen here strongly suggests that they may not be linked, however odd that may be.
Feeling somewhat flummoxed, I asked Dr. Kory - one of the world’s leading pulmonologists who has extensive experience treating ICU covid patients at various stages in the pandemic, and thus uniquely suited to weigh in on this - what he made of these odd findings. He offered the following insights as potential explanations (reproduced with permission & lightly edited for style/form):
“PE’s can often be undiagnosed, especially when they occur in the setting of a severe pulmonary disease”; “sometimes, if the patient is really sick and in shock, you can’t get them to a CT scanner when they are unstable.”
PE’s could be discovered as a Deep Vein Thrombosis (DVT) and treated before they reach the lung and become a PE. (*There isn’t enough of an increase in DVT’s in death certificates during the pandemic years to reach any sort of statistical significance.)
In other words, PE’s that kill you would often go undiagnosed if you had covid; while PE’s that were discovered would typically get treated before the clot became a PE by being “thrown” to the lungs from elsewhere in the body where the clot initially formed.
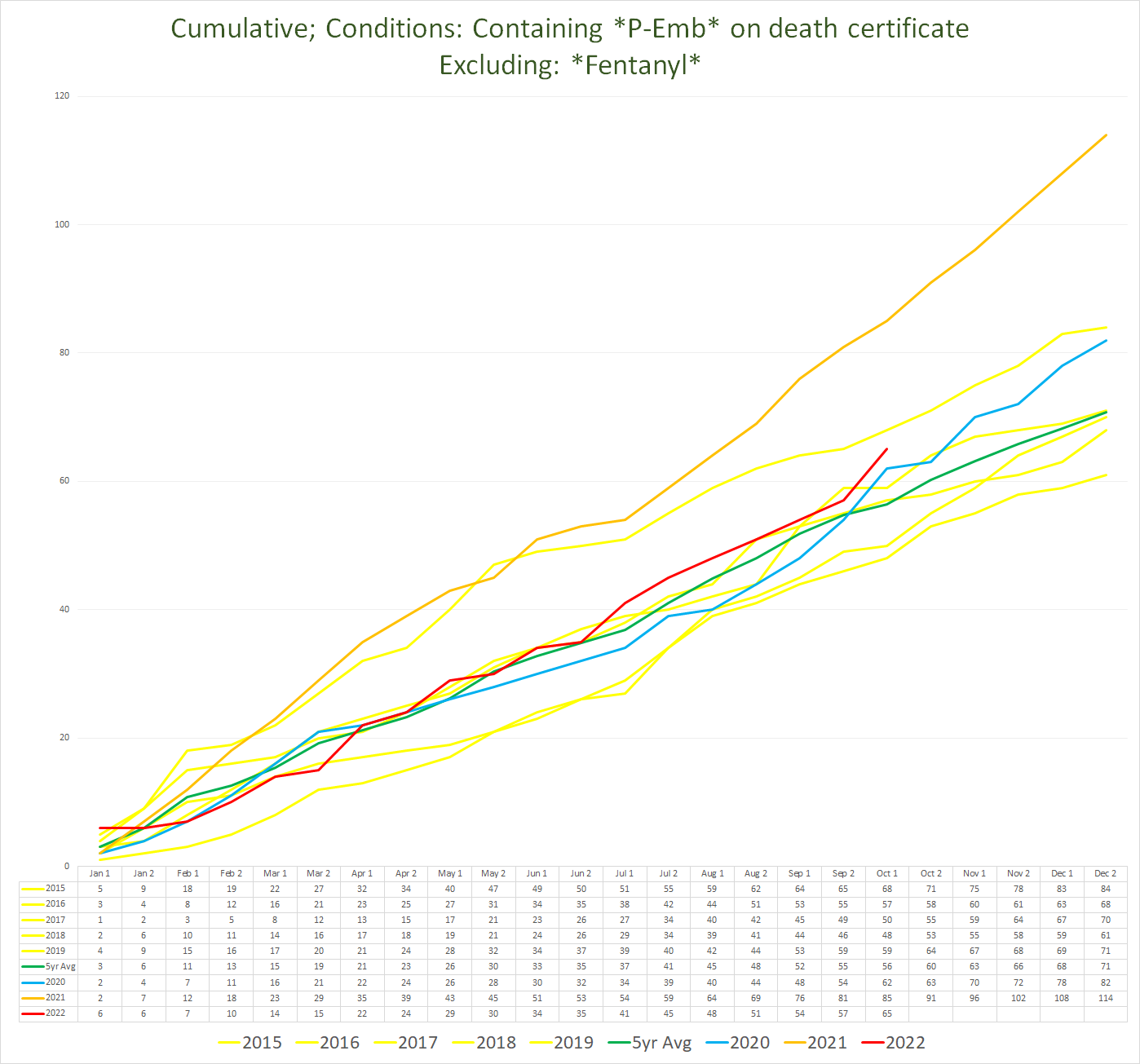
Pulmonary Emboli - 2021
2021 presents a different picture. Unlike in 2020, both genders get hammered (although the ladies maintain an advantage):
The bulk of the runaway increase tracks with covid (based upon the prior analysis above correlating excesses in other respiratory conditions with the excess mortality & covid-labeled deaths starting in late 2021):
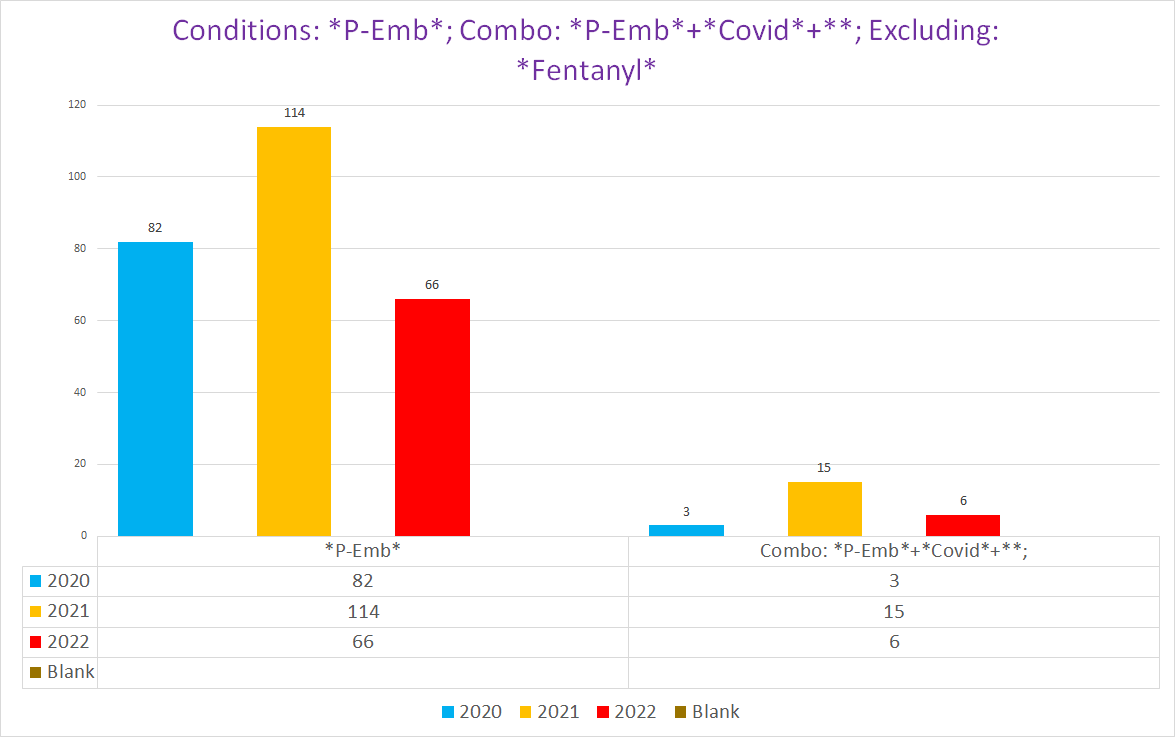
However, the majority of these extra PE’s (left yellow & red columns) do not have covid on the death certificate (right yellow & red columns):
The most plausible and straightforward explanation of this is that the excess PE’s are from a combination of vaccine-enhanced covid disease pathology and vaccine mediated clots. (I am not aware of any proposed theory to explain how pandemic policy-related health issues could manifest as a sudden and abrupt surge in blood clots.) It is eminently reasonable that the vaccines place you at even higher risk of developing blood clots if you get covid (in addition to the clotting risks of the vaccine itself), because you would have the combined clotting potential from both the vaccines and from the covid virus (they do both have those pesky spike proteins).
But maybe for whatever reason, for patients with PE’s that resulted in death, there are covid deaths that weren’t documented on death certificates?
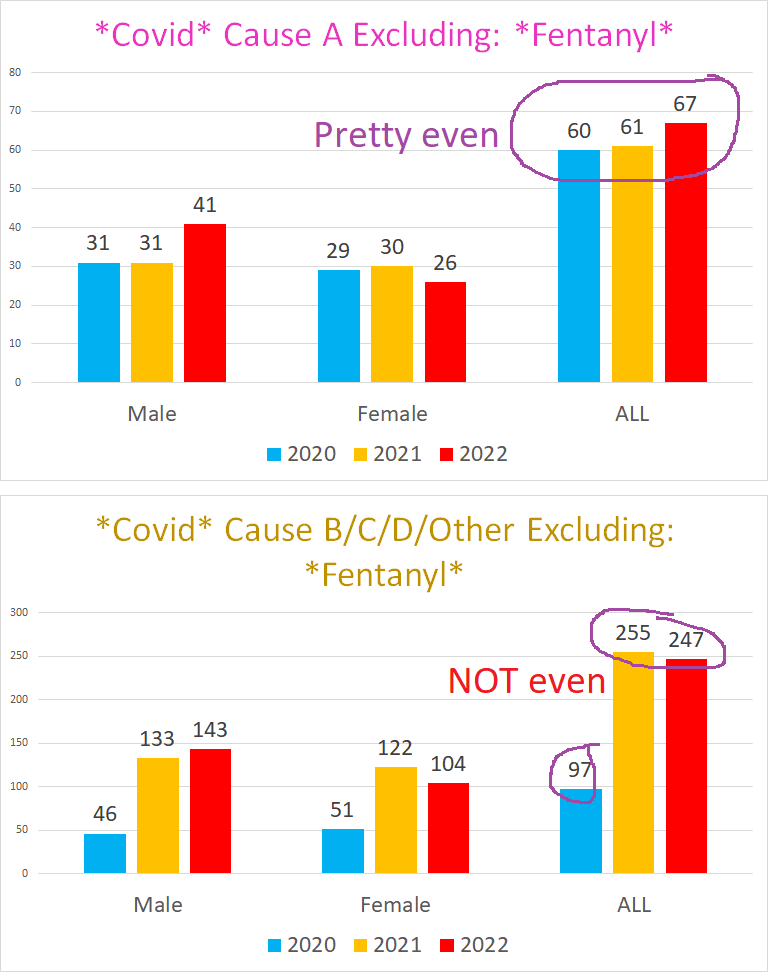
I doubt it. There’s a curious trend from 2020 to 2021/2022 - the proportion of covid deaths that list covid as Cause A vs one of the secondary/underlying causes shifts rather dramatically:
This chart excludes a Fentanyl death where covid was also included as a CoD
The proportion of covid deaths that are listed as Cause A drops from 39.47% (60/152) in 2020 to a paltry 19.81% (61/308) for 2021 and 21.75% (67/308) for 2022. Put differently, the number of Cause A Covid deaths is the same in 2021 as in 2020 (2022 is only through mid-October, so will presumably soundly beat out 2020/2021). The entirety of the increase in covid deaths in Vermont in 2021 over 2020 is in deaths including covid as a secondary or underlying CoD.
Does this mean that all the non-Cause A covid deaths are illegitimate? Nope. Remember, we can see the excess respiratory disease mortality coinciding with the increase in non-Cause A covid deaths (note: these charts are not scaled equally on the Y-Axis):
What this does suggest however is the possibility that deaths were being attributed to covid more liberally after 2020. Thus it is very counterintuitive and unlikely that in 2021 there was a glut of fatal pulmonary emboli caused by acute covid disease that were nonetheless undocumented on death certificates, despite what appear to be looser standards for attributing deaths to covid.
(To be completely honest, there is a possibility that was institutional reluctance to attribute deaths to covid after the mass vaccination of nearly the entire state. Vermont had such a high % of the population fully vaccinated that it may have been intuitively obvious that there could not possibly be a tangible # of unvaccinated covid deaths. In this circumstance, attributing large numbers of deaths to covid could feel like or amount to a de facto acknowledgment of profound vaccine failure.)
What can we derive from this data?
So far, we have established that there was almost definitely a massive, unprecedented surge of deaths involving various respiratory system conditions in Vermont over the last four months of 2021 extending through the whole of 2022 to date.
Can we attribute the late 2021 pandemic of respiratory illness to the vaccine and the vaccinated?
The overwhelming majority of covid deaths (real or imagined) were suffered by the 65+ age cohort - who were 95% fully vaccinated by mid-September 2021, and the rest were in the 51-64 cohort that was at least 82% fully vaccinated by that time:
Ergo, it is mathematically impossible for there to be a sufficient number of unvaccinated covid deaths that could support claims of vaccine efficacy, because they comprise too insignificant a portion of the population. Furthermore, by September 2021, most of the unvaccinated would have already developed at least some immunity to covid from exposure over the past year and a half, immunity which we know actually works. We can thus safely conclude that this was at minimum a pandemic of the vaccinated as much as the unvaccinated.
Did the vaccine make covid disease more virulent and lethal?
It is an objective fact that in Vermont, 2021/2022 covid (or the “respiratory disease pandemic”) was far more severe than 2020 covid. It is likewise an objective fact that the overwhelming bulk of the excess covid mortality in 2021 and beyond occurred after Vermont had achieved nigh on perfect vaccine coverage of the senior population, and over 80% for the remainder of the population that faced any degree of cognizable risk from covid (however slight).
Draw your own conclusions.
Conclusion
It is basic common sense that if the vaccines truly substantially reduced the burden of covid disease, we would see that manifest at least to some degree in the real world.
Covid, we were told, was a once-in-a-lifetime pandemic; we were also told that this epochal plague was neutered by the covid vaccines.
This is a far cry from what is depicted by the all-cause mortality:
The ultimate test of something is how it performs in the real world. We trust the science and technology we use because we can see for ourselves that it works (well, usually anyway).
If the covid vaccines worked as advertised, then how come they don’t work?
Very interesting, especially the male female data as the number one user of jabs are liberal females. Would also like to see the ACM rates as well as birth rates and stillborn rates.















Do the dearh certificates have shot history at all? Is the data you have anonymized or could you get the actual shot history with a list of names?
Very interesting, especially the male female data as the number one user of jabs are liberal females. Would also like to see the ACM rates as well as birth rates and stillborn rates.