
Ivermectin and The Curse of the Covid Illiterati
When Facts and Experts Collide, the Patients Bear the Costs

HT to Caputo, the first part is an attempt to shorten the part of his incredibly well-researched piece depicting the trials and tribulations of the Smentkiewicz family to a manageable length, and without weaving in and out of the storyline.
Judy Smentkiewicz was dying. Sedated and on a ventilator for almost a month in Millard Fillmore Hospital in upstate Williamsville, New York, her doctors had run out of (the precious few) CDC-approved treatment options. Her family was advised that as the odds of her recovering were bleak, they should consider making preparations for what looked to be the grim finality of yet another 80-year-old succumbing to Covid-19. Her children, however, refused to give up; their resolve ultimately saved Mrs. Smentkiewicz’s life. To make a long story short(er), her son Michael’s mother-in-law happened across a YouTube video of Dr. Pierre Kory, a world-renown pulmonologist with numerous papers published across the most prestigious medical journals, which she promptly forwarded along to her son-in-law. In the video, Dr. Kory explained how Ivermectin is a miracle drug in the fight against Covid-19, with an avalanche of data supporting its safety and incredible efficacy at all stages of Covid-19 disease progression. Despite the hospital’s initial refusal, Michael eventually wore down hospital staff to the point that a hospital administrator reluctantly signed off on dispensing Mrs. Smentkiewicz one dose of Ivermectin. Incredulous doctors were shocked when Judy immediately started to improve; less than 24 hours later, she was off the ventilator(!).
This miraculous turnaround stands in stark contrast to the Borg-esque unanimity of the medical community, who constantly, and sometimes very passionately, excoriate anyone who dares to claim that Ivermectin has any efficacy whatsoever in treating covid. It seems as though every (one of the precious few sparse) utterance of the “I-word” on national media and public health agencies ranges from “it doesn’t work” to “it’s an internet conspiracy theory”. I want to draw attention to this sharp and irreconcilable contrast between ‘experts’ and facts; its unresolved dichotomy is my rationale for writing this essay, the main thrust of which will be to present some of the real-world studies and data (see below).
Returning to our shocking vignette, the hospital promptly discontinued the Ivermectin after the one dose, whereupon Mrs. Smentkiewicz started regressing; and despite the desperate pleas from her family that it be resumed, the hospital flatly refused (?!?!?). Even after her family retained counsel and sued in state court, the hospital remained steadfast in its adamant opposition to allowing further treatment with Ivermectin, and instead of just giving a dying woman a drug that literally costs pennies and with a safety profile superior to that of Tylenol, they chose to fight the Smentkiewicz’s in court. The hospital’s lawyers assumed the case would be dismissed as courts typically defer to the expertise of the hospital’s doctors in disputes of medical judgement or fact. Mercifully, they thought wrong. Despite the overwhelming and instinctive reticence of judges to wade into medical decision-making, the hospital’s actions were so indefensible and predacious that a dumbfounded Judge Henry Nowak ordered the immediate resumption of Ivermectin (which was an act of extreme judicial bravery, nonetheless, considering the political climate).
Still, though it seems astonishing and incomprehensible, this was not the end of the Smentkiewicz’s ordeal. The hospital summarily refused to abide by the judge’s order, choosing instead to demand a hearing to determine if a patient has the right to choose their own medicine (a novel radical legal theory that if true would mean that patients don’t have a right to seek a second opinion so long as the patient cannot be moved to a different hospital). In the ensuing hearing before the now completely flabbergasted Judge Nowak, the hospital begrudgingly conceded to allow for the administering of Ivermectin provided that it was prescribed by a doctor outside their network. Judy received her 2nd dose of Ivermectin at 11:00 that night, and for the second time experienced an immediate turnaround; three doses later she was discharged from the hospital.
An almost identical saga played out in Rochester General Hospital a week later, where, like Judy Smentkiewicz, 65-year-old Glenna Dickinson was attached to a ventilator and dying from Covid. Her daughter saw a local news report of Mrs. Smentkiewicz’s miraculous recovery from Ivermectin and persuaded her mother’s regular doctor to prescribe some for her mother.
Who is Mrs. Dickinson’s doctor? That would be one Dr. Thomas Madejski, whose bio includes:
“[sic] internist and chief of medicine at Medina Memorial Hospital, former president of the New York State medical society, a clinical instructor in medicine and pharmacy at the University of Buffalo, who sits on the Board of Trustees of the American Medical Association as an expert in geriatric medicine.”
Clearly, not some anti-vaxxer quack.
Well, as is apparently de regueur in many prominent hospitals, the ICU doctors refused to allow Mrs. Dickinson to even receive the Ivermectin already prescribed and obtained through her regular doctor. Fortunately for Mrs. Dickinson, another judge agreed with her and forced the hospital to administer the Ivermectin, and
“[12] hours later, after one 12 mg dose that her daughter picked up at Walgreens for eighty-three cents, Glenna’s vitals were much improved. She was “completely stable and doing much better,” [her lawyer] Lorigo said. They reduced her ventilator 50 percent, no longer had to “flip” her from her back to her belly for better oxygen flow, and they moved her to a “step down ICU.”
She subsequently recovered sufficiently to be discharged from the hospital.
Yet another instance of this sort of depraved lunacy by medical professionals in direct contravention of the most sacred of medical principles - “primum non nocere” (do no harm) - involved John Swanson, 81, of Genesee County, New York. (New York sure seems to have its share of evil medical practitioners, doesn’t it?) He was
“[sic] on a ventilator at the United Memorial Medical Center in Batavia and, according to the court affidavit, was "on death's doorstep”. The Buffalo News report[ed] that, according to attorney Ralph C. Lorigo, Swanson was given one dose of ivermectin and began breathing on his own, was then taken off the ventilator, and began to show great progress. However, the hospital, with no other legitimate treatment options to offer, refused to give him follow-up doses. On April 2, state Supreme Court Justice Frederick J. Marshall ordered the hospital to administer the follow-up doses at the request of Swanson's wife.”
He, too, went on to recover, no thanks to United Memorial Medical Center.
Reassuring us that rabid anti-Ivermectin policies are non-discriminatory is the case of Nurije Fype, 68, who was placed on a ventilator following cardiac arrest in Edward-Elmhurst Hospital in Chicago. Desi Fype, her daughter, sued in court to compel the hospital to give her mother Ivermectin after the hospital refused and had no other treatment options to offer. As reported by the local Fox affiliate,
An Elmhurst woman whose mother is in grave condition with COVID-19 says a local hospital is refusing to treat her mom with a specific drug, despite a judge's order to do so.
"She might pass away within hours," said Desi Fype of her 68-year-old mom, Nurije, whose condition has been deteriorating since she was admitted to Edward-Elmhurst Hospital on April 7.
This week, they secured a court order from a judge in DuPage County, ordering Edward-Elmhurst Hospital to administer ivermectin to Nurije Fype.
But Fype and her legal team say the hospital didn't budge and continues to refuse to give her mother the drug.
"[The judge] ordered that Elmhurst Hospital and Elmhurst Medical Group to administer ivermectin to the ward, per the prescription, immediately," Lorigo said. "That's what he ordered. That order's properly served on the hospital, and the hospital refuses."
Even after the Fype’s, in order to avoid the stated objections of the hospital that the hospital prescribe Ivermectin, offered to procure the Ivermectin from an outside physician, the hospital refused (!?!?!?!). Ultimately, the court finally prevailed upon the hospital when, as reported by MSN,
DuPage County Judge James Orel ordered Elmhurst Hospital not to stand in the way of Fype receiving the medication. When Fype’s own doctor was unable to administer it, Lorigo said, the legal team found another physician who had to travel “1½, 2 hours each way” but was willing to do it.”
What would have happened had they not found a doctor willing to drive 3-4 hours just to administer a dose of Ivermectin?
These horrifying anecdotes represent the vanishingly small percentage of patients, especially amongst the elderly, who have family members that possess the moxie and mojo to not only do their own independent research against the unified voice of the entire media, government, and medical community; not only go out on a limb to pester the doctors repeatedly over a patient they consider to be a lost cause; not only to stubbornly demand they administer a treatment considered by the proper medical establishment to be voodoo quackery; but to hire a lawyer and sue the hospital in court – a tactic whose failure under normal conditions would be a fait accompli. How many patients in similar circumstances died because they lacked family with this sort of indefatigable relentlessness and intestinal fortitude?
This all begs the question -- why on Earth would hospitals go to court to fight patients they themselves had already given up on, and for whom they had no more treatment options, in order to prevent even outside doctors from prescribing a medication that is safer than Tylenol? I submit that there is indeed something very nefarious afoot here. When British doctors not only wished to take 2-year-old Alfie Evans off of life support – who suffered from a terminal degenerative neurological condition – but also refused to allow Alfie to receive privately funded experimental medical treatment in the US, their naked depravity shocked the world. Now, however, hospitals are content to fight in court to uphold their right to deny potential lifesaving treatment procured and administered by a third party that they acknowledge in court presents no additional risk to the patient, and there is no hubbub about it anywhere. No outrage. No uproar. Nothing. Zip. Zilch. Nada. The foundation for the faith and confidence uniquely attributed to medical professionals in Western societies is rooted in the medical profession’s ethos prizing saving life above all else. This is most certainly no longer the case regarding the medical community writ large. At a minimum, a medical community whose culture breeds such contempt for the value of a patient’s life that they will fight in court to deny potentially lifesaving treatment that is essentially cost-free and without any legal liability is a medical profession that does not have any credibility whatsoever insofar as potential covid treatments are concerned, because there is no presumption (regarding Covid for sure) that their overriding concern is saving lives. And even if they were 100% correct that Ivermectin does not work, what happened to basic compassion for the patient’s family? The very least the hospital could do is give the family peace of mind knowing that at least they tried everything humanly possible (which is significant psychologically). That some medical professionals do not ascribe to such an abhorrent ethos is no defense for believing and parroting the claims promoted by its practitioners.
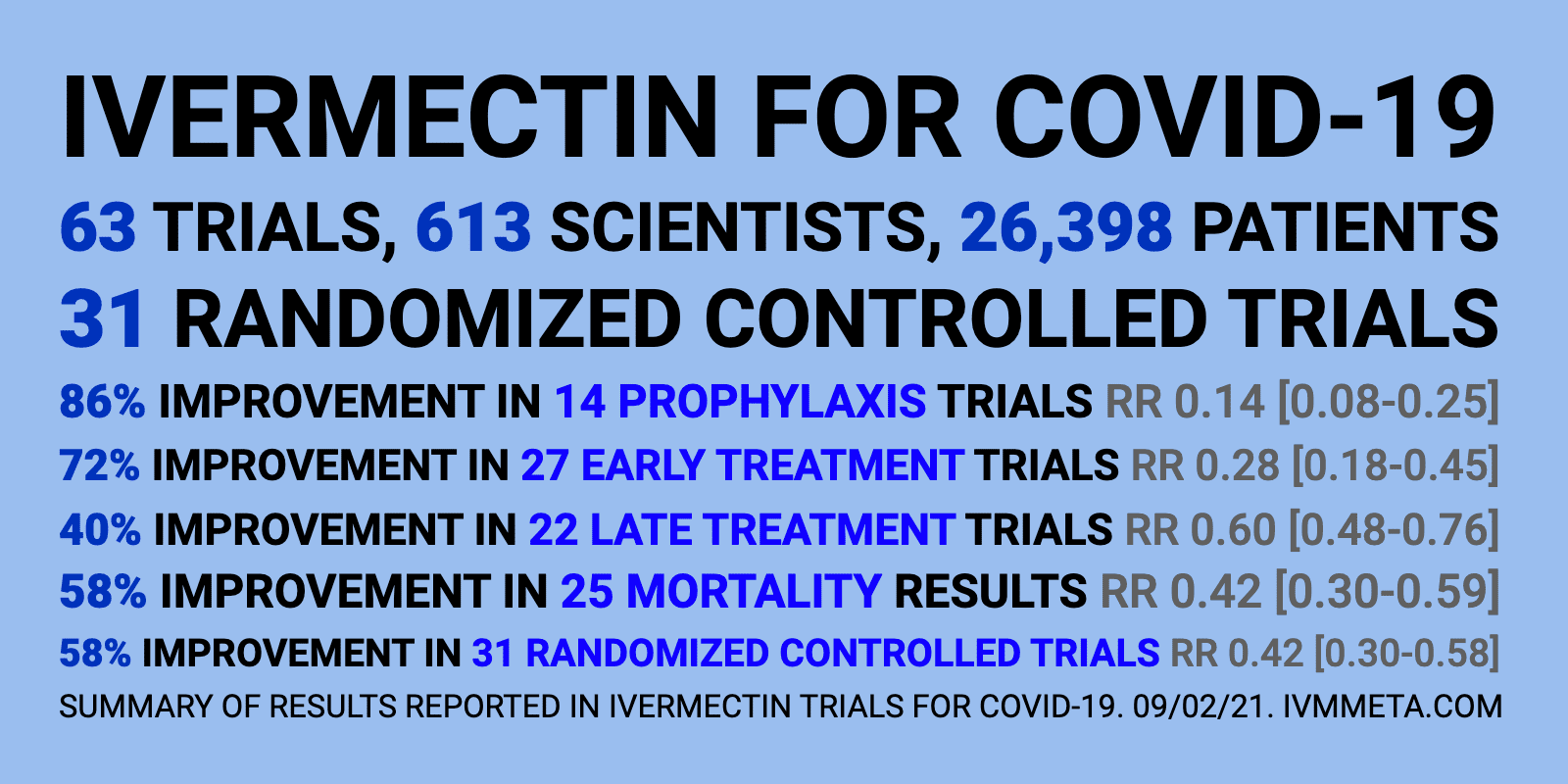
The Ivermectin Data:
The primary objective in writing this article, however, is to present a portion of the actual Ivermectin data showing its efficacy against covid using language and concepts readily cognizable by a layperson without any expertise in the technical formulas of statistical analysis or alien academic vernacular. The vast majority of medical professionals (who has any sort of public platform) have been railing against Ivermectin. They claim that “the science” and “the data” and “the studies” all prove – conclusively, and apparently self-evidently too judging by the acerbic and vitriolic attacks leveled by some - that Ivermectin is a big hoax a la hydroxychloroquine (a subject requiring its own article in this format). I aim to demonstrate their profound ignorance and illiteracy concerning anything to do with Ivermectin, by simply presenting the real-world studies and data so derisively dismissed by the medical ‘experts’, affording everyone the opportunity to see for themselves what the data is and shows without the interlocution of the local doctor-priest. This will hopefully strip this medical incarnation of philosopher-kings of the pretentious façade of expertise to reveal their dangerous ignorance regarding Ivermectin (and the other treatment protocols by extension), that has undoubtedly led to some number of needless deaths in people who would have availed themselves of these treatment options had they not been forcefully dissuaded by one of these well-meaning yet unwitting clinicians.
Before presenting the data, it is necessary to provide definitions for a few intimidating phrases that are unavoidable:
· Random Control Trial (RCT) – a study where the subjects are allocated or distributed randomly between the control group and the treatment group(/s).
· Unblind – the scientists running the study know which subjects are in which group.
· Retrospective – a study that looks at something that already happened.
Here is a summary of just a few of these studies (cherry picked mostly on the basis of containing final results that are intelligible to the layperson):
(Note: The penmanship of pre-print studies can sometimes be a bit shoddy, which is fairly typical for pre-print studies authored by foreign non-native English speaking scientists.)
Prophylaxis:
1- Carvallo et al, Un-random Controlled Prophylaxis, 1195 health care workers (HCW’s), 2 groups, 788 given 1x/week prophylaxis, control of 407 HCW’s. Results: 237/407 (58.2%) lab-confirmed covid infections in control vs 0/788 – ZERO!! - in Ivermectin arm.
2- Morgenstern et al: Observational Retrospective Cohort Study Prophylaxis, HCW’s, 271 Ivermectin arm, 271 control. Results: Ivermectin arm = 1.8% lab-confirmed covid infections vs 6.2% control arm, = 74% reduction in odds of contracting covid. (Also, zero hospitalizations in Ivermectin arm vs 2 in control arm).
3- Guerrero et al, Retrospective Statistical Analysis Compared 31 African countries that use Ivermectin widely already (to combat onchocerciasis (river blindness)) vs 22 that don’t. Results: “In conclusion, in the countries where ivermectin is distributed to and used by the entire areas, it [leads to] a reduction in mortality, to accelerate[d] patient recovery and, [less] death. And this analytical study will suggest that early treatment with ivermectin may accelerate recovery and prevent worsening of symptoms in patients with mild disease. These findings can be efficiently translated into therapies for SARS-CoV-2 (COVID-19).” (The raw numbers are a bit complex, but this is one of the most robust data sets in favor of Ivermectin efficacy, so I included it anyway.)
4- Chahla et al, RCT, Prophylaxis, 234 HCW’s, 117 each arm. Results: Ivermectin arm – 4/117 covid infection, all mild symptoms; Control arm - 25/117, 15 mild symptoms, 7 moderate symptoms, 3 severe symptoms.
5- Carvallo et al, RCT, Prophylaxis, 229 HCW’s 2 groups, Ivermectin arm – 131, control – 98. Results: Ivermectin – 0/131 covid infections vs control 11/98.
6- Shouman et al, Unblinded RCT, Prophylaxis, 304 contacts of hospitalized covid patients, 203 Ivermectin arm, 101 control arm. Results: Ivermectin arm = 15/203 (7.4%) covid infection (8 mild, 6 moderate, 1 severe) vs Control arm = 59/101 (58.4%) (31 mild, 21 moderate, 7 severe). (Quote from the study: “the high protective efficacy detected for ivermectin made the researchers to stop prematurely the non-intervention arm.” (In other words, they decided that it was unethical to not give ivermectin to the control arm too, because of the dramatic effect it was having thus far.)
Treatment:
1- Merino et al., Retrospective Observational Statistical analysis of Mexico City. Population of Mexico City divided into 2 groups: Group 1 = those that got Ivermectin kit, Group 2 = those that didn’t. Results: Ivermectin group 68.4% - 74.4% reduction in hospitalization odds vs non-Ivermectin.
2- Mourya et al., RCT, Early Treatment, 100 hospitalized covid patients divided into 2 groups of 50. Results: After 7 days, 5/50 Ivermectin arm covid positive vs 47/50 in control, = 84.9% less likely to still have covid after 7 days of treatment.
3- Emmerich et al., Comparisons between the Neighboring States of Amazonas and Pará in Brazil. Baseline – May 2020, deaths = 15.7 (Amazonas) vs 17.1 (Pará) deaths/million/day [before Ivermectin]. Results: accumulated mortality per population from 11/11/2020 to 3/15/2021 of Amazonas (anti-Ivermectin) and Pará (used Ivermectin) are 1645 (Amazonas) and 296 (Pará) deaths/million, = Ivermectin state had less than 1/5 of the mortality of the neighboring non-ivermectin state.
4- Chamie-Quintero et al., Observational Retrospective Temporal Analysis of Peru comparing mortality when Ivermectin was permitted vs when it was subsequently restricted. Results: Ivermectin use in Peru led to 14x reduction in mortality vs Ivermectin restrictions led to subsequent 13x rise in mortality. (There is more specific data in this study that is highly demonstrative of Ivermectin’s efficacy, but it would be too long to put it all here.)
5- Lima-Morales et al., Unblinded Control Study, 768 symptomatic covid patients, 481 in an Ivermectin+ protocol vs 287 in control. Results: Control – 89/287 (31%) hospitalized, 52/287 died (18.1%), 169/287 (58.9%) recovered ≤14 days vs Ivermectin – 44/481 (9.1%) hospitalized, 15/481 (3.1%) died, 406/481 (84.4%) recovered ≤14 days. = Ivermectin 77.7% reduced risk of death and 67.4% reduced risk of hospitalization.
6- Budhiraja et al., Retrospective Observational Study 976 hospitalized Covid patients, 34 treated with Ivermectin. Results: Control – 103/942 died, Ivermectin – 0/34 died.
Finally, here is the conclusion one of the meta-analysis studies, the lead author of which is the world’s pre-eminent Ivermectin-Covid expert/advocate, reviewing the totality of the Ivermectin literature:
Therapeutic Advances:
A large majority of randomized and observational controlled trials of ivermectin are reporting repeated, large magnitude improvements in clinical outcomes. Numerous prophylaxis trials demonstrate that regular ivermectin use leads to large reductions in transmission. Multiple, large “natural experiments” occurred in regions that initiated “ivermectin distribution” campaigns followed by tight, reproducible, temporally associated decreases in case counts and case fatality rates compared with nearby regions without such campaigns.
Conclusions:
Meta-analyses based on 18 randomized controlled treatment trials of ivermectin in COVID-19 have found large, statistically significant reductions in mortality, time to clinical recovery, and time to viral clearance. Furthermore, results from numerous controlled prophylaxis trials report significantly reduced risks of contracting COVID-19 with the regular use of ivermectin. Finally, the many examples of ivermectin distribution campaigns leading to rapid population-wide decreases in morbidity and mortality indicate that an oral agent effective in all phases of COVID-19 has been identified.
Two major meta-analyses were published very recently, both conducted by WHO expert consultants, using the highest standard of statistical analysis (Cochrane test). They found that Ivermectin significantly reduced all metrics of covid incidence and severity:
Bryant et al: “Moderate-certainty evidence finds that large reductions in COVID-19 deaths are possible using ivermectin. Using ivermectin early in the clinical course may reduce numbers progressing to severe disease. The apparent safety and low cost suggest that ivermectin is likely to have a significant impact on the SARS-CoV-2 pandemic globally.” (Moderate certainty evidence is a technical term of art, not a measure that the evidence is significantly lacking.)
The lead researcher for Bryant et al, Dr. Tess Lawrie, stated that she never saw an evidence base anywhere near this robust be ignored in all her decades analyzing studies for various topics and drugs.
Hill et al: “Results: Ivermectin was associated with reduced inflammatory markers (C-Reactive Protein, d-dimer and ferritin) and faster viral clearance by PCR. Viral clearance was treatment dose- and duration-dependent. Ivermectin showed significantly shorter duration of hospitalization compared to control. In six RCTs of moderate or severe infection, there was a 75% reduction in mortality (Relative Risk=0.25 [95%CI 0.12- 0.52]; p=0.0002); 14/650 (2.1%) deaths on ivermectin; 57/597 (9.5%) deaths in controls) with favorable clinical recovery and reduced hospitalization.”
It is true that for most (although definitely not all) of these studies, were they the only one, or one of a few, are too small, or didn’t eliminate all of the potentially confounding variables in play, and would thus be too unreliable for anything beyond conjecture and speculative guesswork. However, a large number of individually weak studies all yielding the same result is itself strong evidence, because the odds of running 50 or 100 small studies with widely ranging characteristics that all produce the same result are infinitesimally small if their results are random and untrue. That the ‘center of gravity’ of the cumulative Ivermectin studies has remained anchored in place despite the steadily increasing number of RCT’s and other studies conducted is further proof that the studies – collectively - are not significantly biased. (That was for data nerds.)
One final but crucial point is that as a general rule, a clinical study will not capture the entire potential effect of a treatment. This is because a study, by its very nature, is a rigid one-size-fits-all (in order to reduce the potential of confounding variables) – everyone gets the exact same dose of the exact same drugs and does not get any other treatments whatsoever. A practicing doctor, on the other hand, has the flexibility to tailor a treatment to a specific patient. Clinical expertise also yields additional specific knowledge not often fleshed out by a study as to what factors are the cause of discrepancies between the majority for whom a treatment is successful versus those for whom it is not, which then further informs the clinician’s subsequent treatment protocols. The upshot of this is that Ivermectin is even more effective than the already extreme efficacy exhibited by the aforementioned studies when prescribed by a trained clinician who understands its use and can tailor the dosage and complementary drug protocols to the specific patient.
Clinical Experience – An untold number of doctors around the world have been successfully treating covid patients with Ivermectin:
How would such data inform the clinical behavior of a rational doctor committed to saving every life in his care? One of many formerly foundational medical principles that has fallen by the wayside during the Covid-19 pandemic is the notion that doctors treat patients using their best clinical judgement when confronted with an unfamiliar pathogen as opposed to waiting for the academic literature to “catch up” to the novel disease. I have been on zoom meetings with doctors that have collectively used Ivermectin to treat, literally, tens of thousands of covid patients, in addition to providing consultation to doctors worldwide who using their protocols and knowhow triumphantly saved hundreds of thousands – if not millions - more. Many of these patients had significant risk factors or were already in the throes of severe covid disease. These doctors/clinicians are not only unimpeachably credentialed, but are among the pantheon of medical revolutionaries who already were responsible for transformative medical breakthroughs. (You can look them up on the FLCCC website.) Various doctors representing a wide array of countries have collaborated to develop and refine different multi-drug protocols centered on Ivermectin (such as I-MASK+, I-RECOVER, and MATH+) through the (formerly ubiquitous) tried-and-true process of trial and error, which they shared with colleagues and physicians around the world who were able to replicate their results. The hundreds, and probably thousands, of doctors worldwide who have utilized Ivermectin so effectively is the most compelling evidence of its efficacy, while paradoxically being the least documented. (Studies are generally a prohibitively expensive enterprise, foreclosing the prospect of random doctors conducting and producing such ventures, however diligent and determined they may be.) I cannot fathom a rational explanation as to why not a single Jewish medical professional that has a public platform (so far as I can tell) has at least consulted with one of the world-renowned doctors or clinicians who have been publicly using Ivermectin, such as Dr. Paul Marik or Dr. Pierre Kory. Email has long since ceased being a novel technology beyond the capacity of otherwise highly skilled medical practitioners to adapt to. Everyone loves to claim that they are committed to transparency. So how come precious few more mainstream individuals have not interviewed one of these brilliant medical luminaries on any of their various platforms?
Coming back full circle to where we started, it is telling that every time a court ordered ivermectin administered to an otherwise terminally ill patient - and it was administered properly - the patient ultimately recovered (as of when this was written). I wonder how many people in various communities sought advice about the prudence of utilizing Ivermectin (or another of the various effective Covid treatment protocols) from their trusted family doctor or other medical professional, and subsequently he/she (or a family member) died from Covid needlessly.