


Explaining the Mechanistic Plausibility for Side Effects, Including Potential Infertility
Manufacturers of biological agents carry the burden of proof that their product does not cause harmful side effects, even speculative ones

Regrettably, experts seldom recognize the limits of their expertise, and vis-à-vis covid seem unaware that any exist altogether.
The following is excerpted from a response written against an article by a specific doctor in my community (whose name I replaced with ****** since there is no need to publicly attack him in this forum):
Dr. ****** claims that there isn’t widespread documentation of a massive quantity - incorporating a wide array – of side effects. He further claims that there is neither a basis nor a plausible biologic theory to sustain legitimate skepticism that the vaccines may cause fertility problems. While I don’t doubt that Dr. ****** sincerely believes his assertions, they do give a distinct impression of the typical unwarranted hubris endemic to scientists, which is an apt description for whomever is ultimately the provenance of these assertions. We shall demonstrate that there are multiple viable mechanistic options for causing a vast assortment of severe adverse effects, including infertility.
Drumroll. . . . . . . . . . . . . . .
At least two foreign, hitherto-undeployed biological entities are introduced to the human body by the covid vaccines (1 in the case of J&J) – the lipid nanoparticle and the spike protein. Common sense cautions that a novel foreign biological substance inserted into the human body may disrupt normal biological functions. This by itself already exceeds the low bar of ‘plausibility’. An analysis of both however will indicate that they are not only ‘plausible’ but likely to cause widespread harm including to reproductive capacity.
Lipid nanoparticles (LNP’s) have long been recognized as highly reactogenic and possessing a variety of toxicological characteristics across various configurations, which was a primary consideration when determining – that is to say, limiting - vaccine dosage. An early hurdle (after the breakthrough discovery of replacing uridine with N1-Methyl-Pseudouridine made the mRNA essentially “usable”) that stymied mRNA research was arranging a molecular structure for the LNP that was not [lethally] toxic. (Many animals ultimately gave their lives in pursuit of this achievement.)
Vaccine proponents claimed that the LNP’s would remain around the injection site, that the spike proteins wouldn’t escape the cells producing them, and that they lacked pathogenicity in any event. Unsurprisingly, none of these claims are true.
Pfizer’s pre-clinical bio-distribution study on the vaccinated animals (released by the Japanese government) found that high quantities of LNP’s accumulated in various organs and tissues, including the ovaries and uterus, and accumulation was vastly disproportionate in the ovaries compared to most other organs (the liver (not shown) and spleen were even more LPN-friendly):
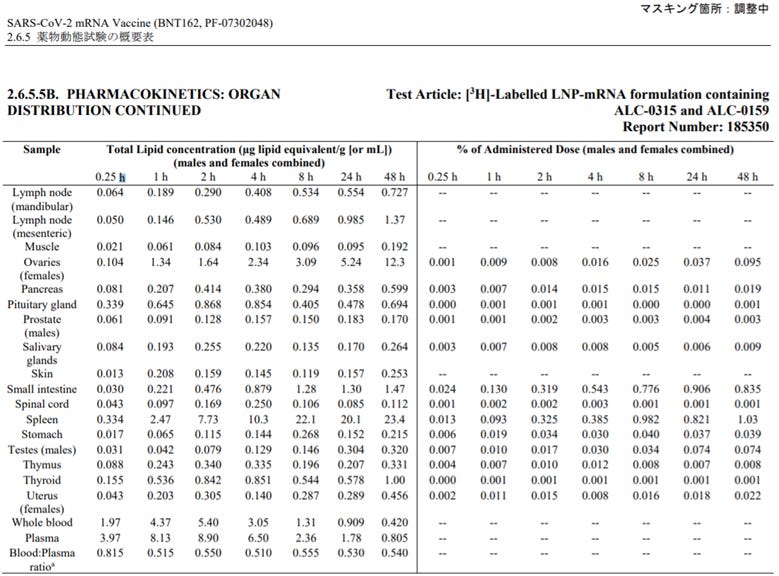
(This result was derived using the lowest sensitivity test, which shall be further discussed below.) A sizeable quantity of a highly reactogenic (picture something that ‘offends’ and ‘triggers’ the immune system) biological agent amassing in any organ system is obviously troubling. Besides for their potent reactogenicity, this suggests a discrete possibility that mRNA may have been intruded into organ tissue cells – which would then produce spike proteins per the vaccine’s design. These cells would subsequently present antigenic Spike proteins, precipitating an immune system attack upon some of the organ tissue directly. Needless to say, a sizeable quantity of a highly reactogenic biological agent amassing in the ovaries doesn’t merely provide mechanistic plausibility for alleged fertility complications, it frankly predicts such injuries to occur. Also needless to say, the thought of, say, heart muscle cells or kidney cells producing spike proteins is a shuddering prospect whose mere utterance requires no supplementary explanation.
A second plausible mechanism for vaccine side effects, including fertility injuries, is the spike protein itself. A recent Oxford study found spike protein circulating in the plasma in 11/13 vaccinated individuals studied, including detached S1 subunits in some. Although not a technical requirement for vaccine approval, bio-distribution studies are considered de regueur, and considering the novel architecture of the covid vaccines, the decision to forgo conducting one is highly suspect. (As spelled out by Dr. Robert Malone, proper bio-distribution study necessarily entails fully dissecting vaccinated animals to extract tissue samples from its entire anatomy, not the notoriously inadequate Luciferase bioluminescence assays they performed for the FDA.) This observation was articulated in the BMJ by one of their senior editors. (Other extraordinarily unusual decisions made running the vaccine trials include excluding all demographics at substantial risk from covid and unblinding and de-controlling the studies by vaccinating the control arms(!!!), a move that forecloses the possibility (read: threat) of high-powered long-term safety data emerging. Ever.) This demonstrates why we don’t rely on scientists claims of “implausibility” – they are too often encumbered by unimaginative thinking and inflated egoism – and this is clearly demonstrated through their ‘anchor’ modification, which ‘unexpectedly’ failed to prevent the mass exodus from their progenitor cells. Regardless, it is undeniably eminently plausible that spike proteins may circulate in significant numbers.
Native S-protein has likewise been firmly established to possess genuine pathogenic traits, which lacking toxicological assessment are presumed to be uninhibited by any of the novel modifications of the vaccine’s adaptation. In SARS-CoV-2 Spike Protein Impairs Endothelial Function via Downregulation of ACE 2, the authors found exactly what the title suggests, namely that merely binding to ACE2 receptors without executing any further pathogenic function disrupted numerous biological processes. (This was an ingeniously crafted experiment, where the researchers grafted S-proteins onto a pseudo-virion platform and infected cute Syrian hamsters with their Frankenstein pseudo-virus, whose sole potentially pathogenic attribute was the ability to bind with cellular surface proteins.) A study published in Nature Neuroscience found that lab animals injected with spike protein into their bloodstream developed cardiovascular problems. More horrifyingly, they also discovered that S1 subunits can cross the blood-brain barrier (BBB), potential triggering all sorts of neurological adverse effects like the large assortment found in the various pharmacovigilance databases. Critically, none of the vaccine makers actually demonstrated that the vaccine’s versions of the spike protein was cured of toxicity or pathogenicity (remember, the point of a vaccine is that you get injected with a dead or inert virus/part of the virus, not the virus’ active ingredient in a fully functional form). It is a small step, not a giant leap, to conjecture that nomadic spike proteins journeying to other organ systems, including reproductive organs, may bind with the ACE2 receptors ubiquitous throughout almost every organ system in the body, again including reproductive organs. Furthermore, incredibly immunogenic spike proteins could conceivably induce a potent immune response wherever they accumulate, leading to inflammation or other detrimental effects in (previously) healthy tissue (or trigger another unknown and unanticipated biological process exerting a detrimental impact)… This, too, easily eclipses the low hurdle of plausibility. Uh-oh, anyone?
As the shocking nature of the revelations just divulged poses a formidable obstacle to most people who have until now only heard widespread claims of properly determined safety by the FDA and other regulatory bodies, it is necessary to provide the specific failures of the FDA in approving these vaccines.
It is instructive by way of introduction that the development timeline was severely truncated while under unprecedented moral, social, and political pressures. A layman readily intuits from this simple fact with common sense derived from all of human history a cautionary signal of hasty decision making inadequately accounting for numerous considerations, of which many are far from obvious, especially to a stressed and burdened mind. It is axiomatic to human nature that commensurate with increasing urgency amid ongoing devastation is an increasing tolerance of risk and corner-cutting, because a rational risk/benefit analysis properly concludes that “desperate times call for desperate measures”. A consistent outgrowth of such circumstances is the predilection to allow such a mindset to persist even in the subsequent absence of its precipitating conditions. This possibility is amplified where previous decisions in hindsight seem unjustified; and becomes probable where previous decisions created a systemic flaw still present which would require not only the embarrassing admission of error but potentially vitiating significant progress towards an unachieved objective, such as the development of a covid vaccine. To pretend otherwise is to be willfully and delusionally ignorant, which is of course the (ill-) considered position of the medical community. We shall provide a few examples of specific decisions that are manifestly defective.
For this, I will simply paraphrase Robert Malone, the first person to synthesize mRNA that successfully infiltrated a cell. The following comes from an interview with Daniel Horowitz (the first one):
The FDA involved only their vaccinologists, leaving out the gene therapy experts. The predictable result was that since traditional vaccines don’t undergo assessment to characterize the duration, distribution, or levels of expression of any component, nor do they undergo reproductive toxicology or genotoxicity, the covid vaccines were spared such testing despite being gene therapies where such enquiries are germane to their safety profile. Thus, the FDA never required that vaccine developers rigorously characterize level, duration, or distribution of manufacturing of spike proteins, or the distribution and toxicology of novel lipid compounds used to construct the LNP delivery vehicle. The meager animal bio-distribution study that was conducted by Pfizer used the least-sensitive testing mechanism. To assess bio-distribution, they coded for Luciferase in the mRNA, a bioluminescent protein responsible for the glow of a firefly’s tail. To analyze the biodistribution of luminescent proteins, they used photon multiplier tubes on whole animals, the least sensitive way of testing, since biological tissues deflect or refract photons, preferentially favoring extremely high concentration areas that are close to the surface. Unsurprisingly, the injection site accounted for the vast majority of the detected luminescence. Proper protocol – which would have been insisted upon had gene therapy experts been consulted – calls for dissecting the animals, extracting samples from the entire anatomy, which are then put in tubes with a buffer, followed by lysing (popping open) the cells and obtaining a sample which is tested for luminescence. This would indicate accurately how much of the mRNA-encoded protein was synthesized in each anatomical sample. That the FDA et al accepted the lowest sensitivity test, reveals their cluelessness in assigning inadequate standards for assessing these vaccines.
Furthermore, the spike protein isn’t the only potential vaccine target antigen, and may not even be the best one. Spike protein itself has many mechanisms that could be targeted besides for the RBD “which could’ve been left in a native structure” [ie, “closed conformation”, in other words, they chose to lock the S1 in an ‘open conformation’, which would keep the RBD exposed, but also enhances ACE2 binding affinity]. Covid contains other proteins that elicit cytotoxic T-Cell lymphocytes [those are the assassin T-Cells that destroy infected cells]. Hasty decision making for vaccine development led to ill-considered and harried decisions to target the easiest candidate without considering other implications.
Pfizer explicitly acknowledged in their clinical protocols that reproductive toxicity wasn’t studied in their animal trials.
As far as the LNP’s are concerned, new compounds contain inherently plausible risk that can be retired only through proper trials designed for that specific purpose, something manifestly absent from the trial protocols.
The FDA and vaccine manufacturer’s obviously cut corners in the development and trials of these vaccines.
Other mechanistic theories for vaccine induced injuries is explored in great depth in Worse Than the Disease? Reviewing Some Possible Unintended Consequences of the mRNA Vaccines Against COVID-19 (whose original link seems to have gone offline… gee, I wonder why…), whose abstract includes:
We then review both components of and the intended biological response to these vaccines, including production of the spike protein itself, and their potential relationship to a wide range of both acute and long-term induced pathologies, such as blood disorders, neurodegenerative diseases and autoimmune diseases. Among these potential induced pathologies, we discuss the relevance of prion-protein-related amino acid sequences within the spike protein.
Remember, it’s on vaccine manufacturers to prove that their product is safe, even from highly speculative dangers.
I think a final point is in order concerning Dr. ******’s claim that there is “no plausible biologic theory” that these vaccines can affect fertility. Frankly, such a claim does not possess legs to stand upon even unchallenged by contra-indicating evidence. Were scientist’s inability to conceive of a plausible mechanism for speculative harms a viable standard to adjudicate safety concerns, the FDA could be largely retired, what with little need for the robust testing regiment all novel therapies and biological agents are subjected to in the face of oft theorized lack of plausibility for unexpected adverse effects to occur. Such proclamations are critically examined precisely because we (properly) accord due deference to humanity’s eternal burden of not knowing what we don’t know. Regrettably, experts seldom recognize the limits of their expertise, and vis-à-vis covid seem unaware that any exist altogether.
Additionally, the manifest ignorance of the academic medical community regarding the vaccine embodied in the aforementioned erroneous claims is broadly indicative of this endemic narcissistic egoism. As has been widely disseminated by now, pharmacological surveillance systems worldwide have been capturing wildly unprecedented numbers of Serious Adverse Event (SAE) reports. This is also despite the best efforts of the medical community to dissuade people and medical personnel from reporting adverse incidents, and despite the cumbersome and difficult process to file a VAERS report, and despite the legal threats of federal prosecution ominously restated every time you have to click to advance to the next page.
While it is extremely difficult to peg even a rough estimate of the actual # of SAE’s suffered post-vaccination, it is undeniable that there exists ample and obvious mechanisms by which the vaccines could easily inflict such injuries.
Just a heads-up: Your link points to an Oxford study, not Harvard. Thanks for your work!