


Excess deaths involving blood disorders in Minnesota that began after 2020

One of the medical categories where the excess mortality is elevated by multiple sigma’s or standard deviations (i.e. the degree of variance from the norm) is conditions and disorders of blood & what are termed ‘blood-forming organs’ (ICD 10 codes D50-D89).
The aim of this article is to highlight a few of the more significant ICD codes where the excess in 2021 and/or 2022 above 2020 is stark and readily apparent:
ICD D50 - Iron Deficiency Anemia
ICD D61 - Other Aplastic Anemias
ICD D62 - Acute Posthemorrhagic Anemia
ICD D64 - Other anemias
ICD D65 - Disseminated Intravascular Coagulation
ICD D685 - Primary Thrombophilia
ICD D689 - Unspecified Coagulation Defects
Note #1: Deaths where the UCoD is ICD codes X4, T4 or T51 are excluded from all tallies in order to exclude drug and alcohol OD’s from creating a misleading appearance of excess deaths in other conditions where they are likely incidental to the OD (“died with”).
Note #2: I am only highlighting trends where there is clear excess, so if there is excess death only within a demographic subset such as gender or age cohort, I’m only including the relevant subset.
ICD D50 - Iron Deficiency Anemia
Iron is a critical component of hemoglobin, the protein in red blood cells that binds to oxygen. Without functioning hemoglobin, red blood cells can’t carry oxygen.
Iron deficiency anemia is the condition where you have a shortage of ‘healthy’ red blood cells that have functional hemoglobin proteins. Imagine if there was a severe shortage of the trailers that are attached to the trucks (the part that contains the stuff being carried around), that left half of the truck cabs without a trailer to haul around. Same idea here.
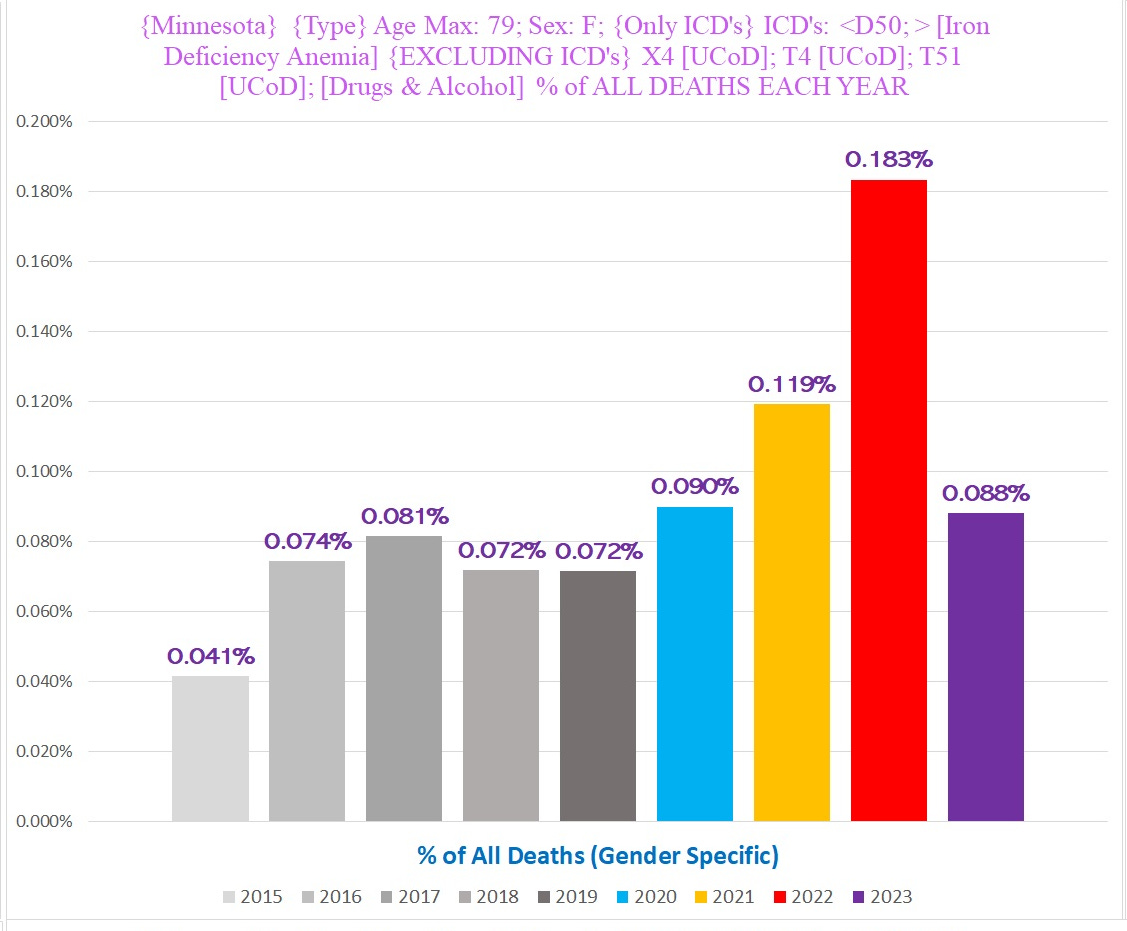
The following chart shows the total number of deaths in females ages 0-79 where Iron Deficiency Anemia (IDA) is identified as a CoD:
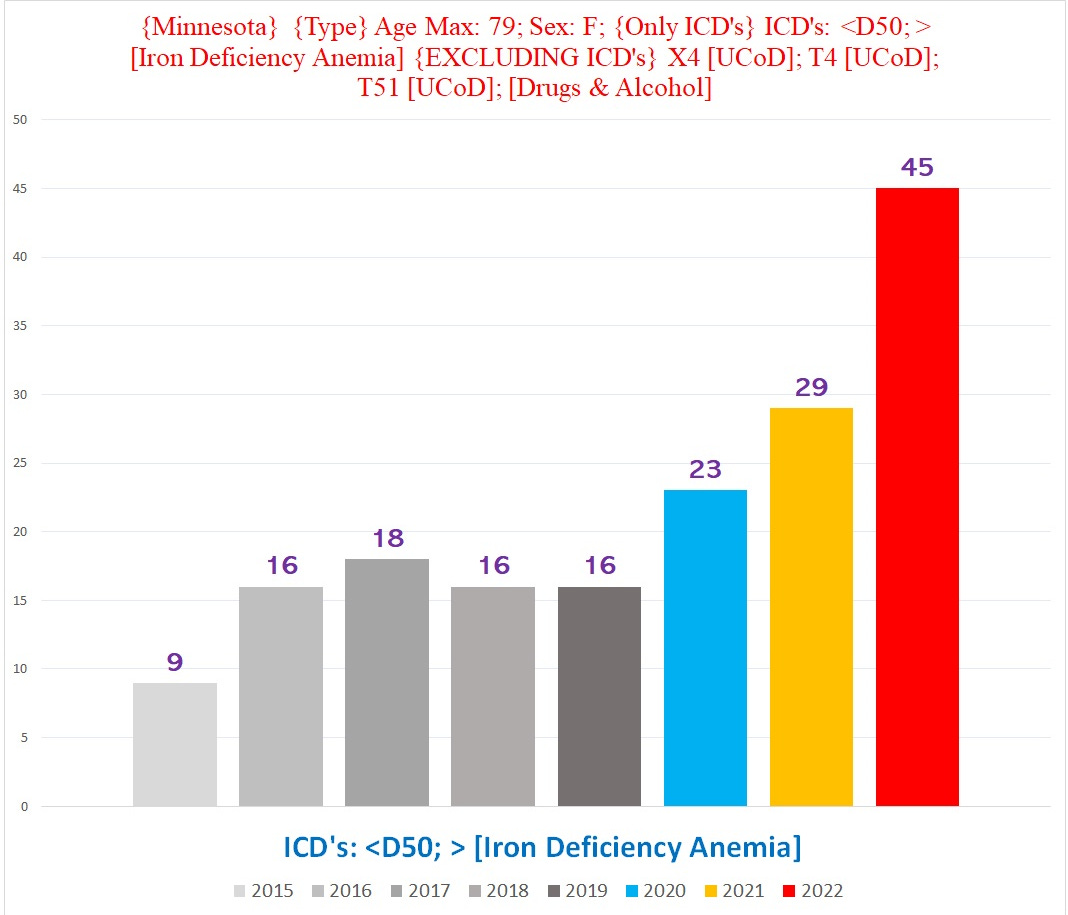
2022 is almost 300% above the pre-pandemic baseline of about 16.
These are not covid deaths - only FOUR even list U071 as the UCoD.
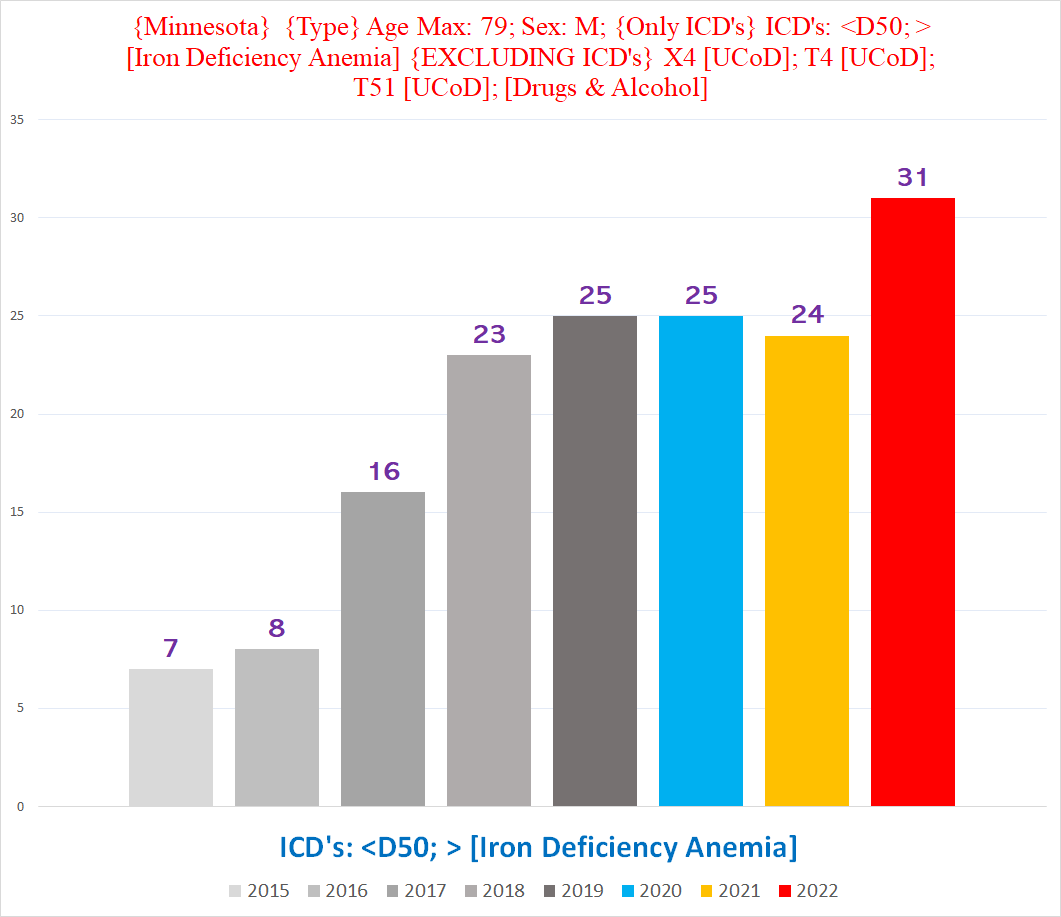
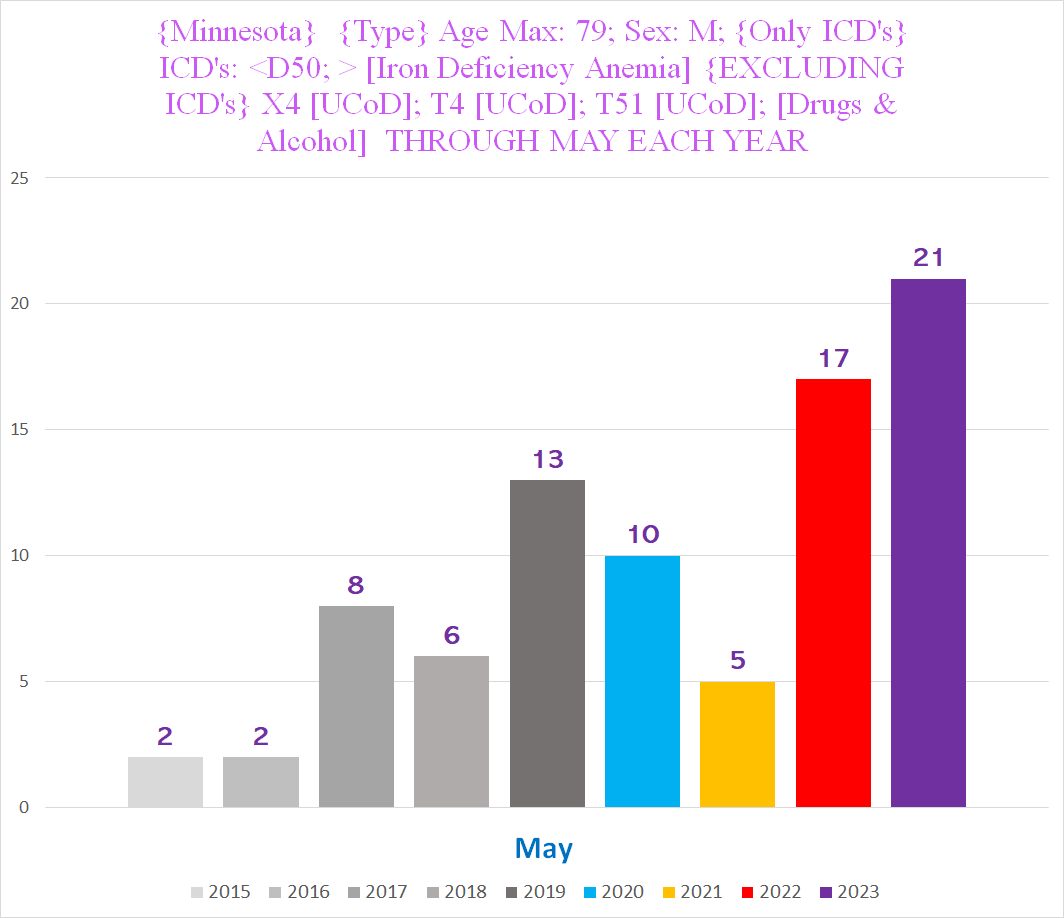
Although the excess in 2022 is less pronounced in the men (ages 0-79) -
- in 2023, the men so far look like the women did in 2022:
The scope of the 2023 deviation is illustrated by the % of all deaths in this cohort that have IDA as a CoD:
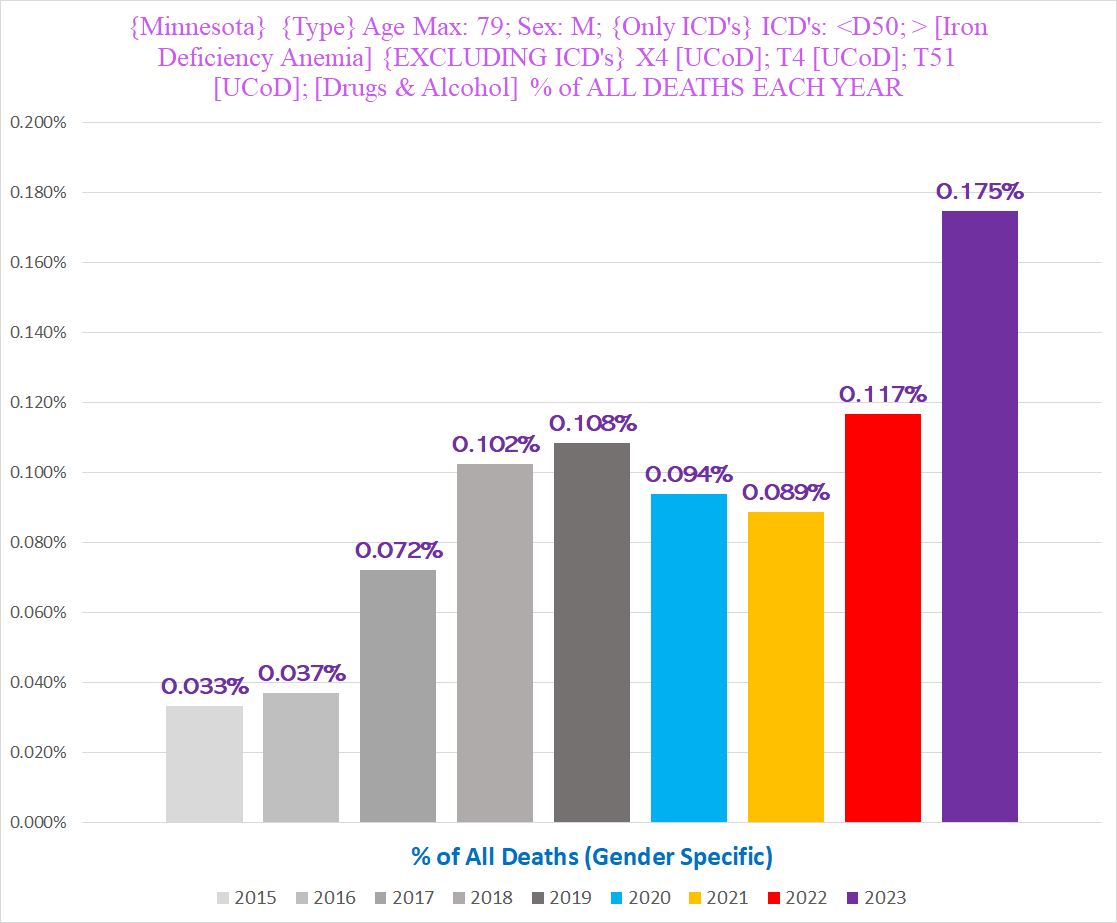
The same pattern is seen with the women, where the % of deaths that have IDA as a CoD skyrockets in 2022:
Clearly, there is or was marked excess mortality with IAD.
ICD D61 - Other Aplastic Anemias
Aplastic Anemia is a condition where your bone marrow can’t produce enough new blood cells. Since blood cells like almost all cells in the body have a finite lifespan (for instance, red blood cells average about 120 days and white blood cells overall average about 12-20 days), the bone marrow needs to be constantly making new cells to replace the old ones as they are removed from circulation (usually through being ‘eaten’ by a type of immune cell called a macrophage or phagocyte).
Like Iron Deficiency Anemia, Aplastic Anemias afflicted primarily seniors (all charts show deaths for ages 65+):

The degree of excess in the topline numbers is not entirely clear, because there is also a pre-pandemic trend in 2018 & 2019 where the number of deaths was rising well above the natural increase of all deaths year over year.
However, if we look at the timing, there is unmistakable excess above pre-pandemic years in Q1, Q2 and Q4:

We see a clear harbinger of excess in the % of all deaths that have Aplastic Anemia - observe how the % in 2022 jumps more than 18% above the % in 2021 after four consecutive years where it was rising by ~1-8% (and the difference year over year weas dropping each year):

This looks like one of the codes where either coroners became more attentive to including it on death certificates and/or the CDC tweaked their algorithm to code a wider set of text descriptions as D61. The % in 2018 jumps 35% over 2017 despite NO excess death in 2018 overall. This also suggests that the excess Aplastic Anemia deaths in 2020 & 2021 could just be an artifact of the overall excess deaths inevitably catching a few people with a pre-existing aplastic anemia condition (if having an aplastic anemia made you more likely to die than the average person in 2020 or 2021, then we would typically see this manifest as an increase in the % of deaths that have an aplastic anemia).
Contrary to 2020/21, the excess in 2022 and the first five months of 2023 seems more likely than not to represent a clinical rather than administrative phenomenon, especially for the women.
Stratified by gender, there is a stark difference between 2022 and 2023. The women had escalating excess every year starting in 2020, but it explodes in 2023:

On the other hand, for the men, 2023 is trending below 2022:
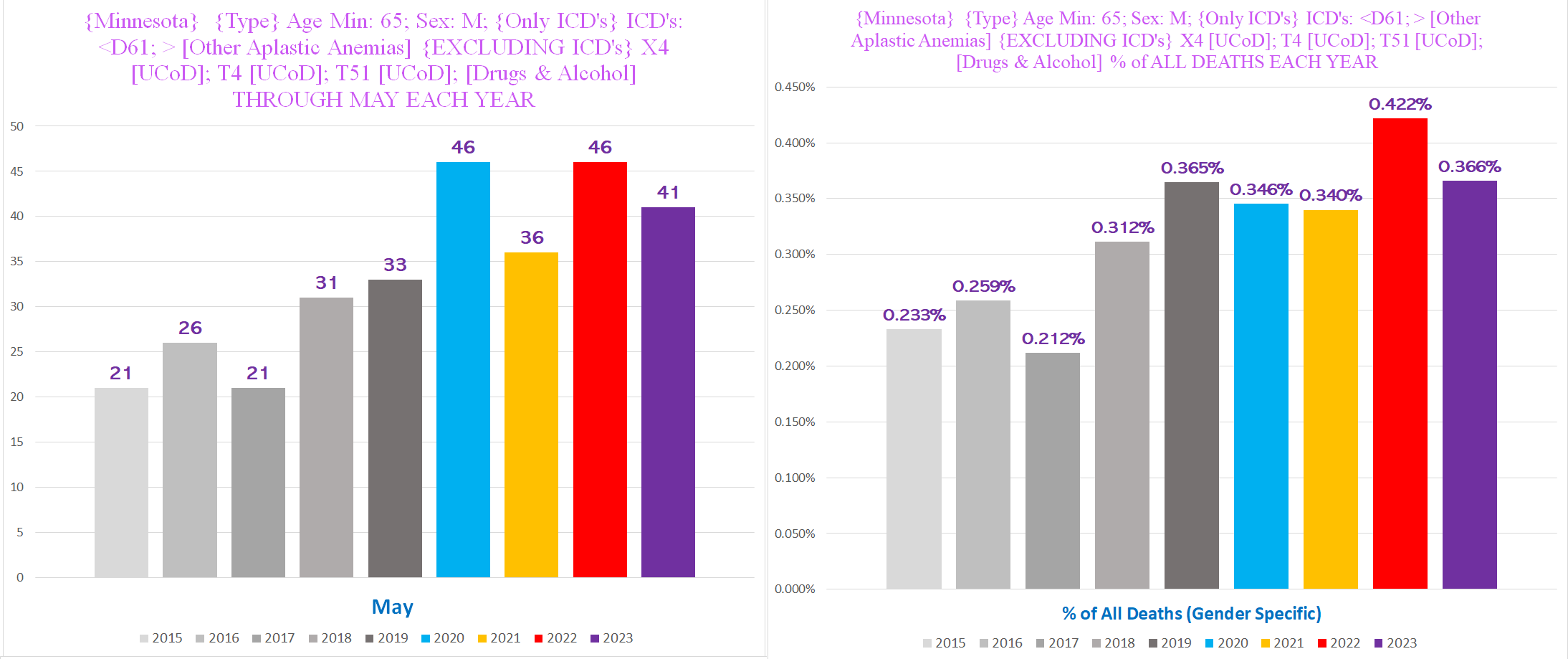
(The 2020 excess for the men looks to be largely a bunch of extra ‘died with’ - the % of male deaths with D61 actually decreases in 2020 compared to 2019.)
Either way, there certainly seems to be excess mortality in 2022 and 2023 depending on which gender.
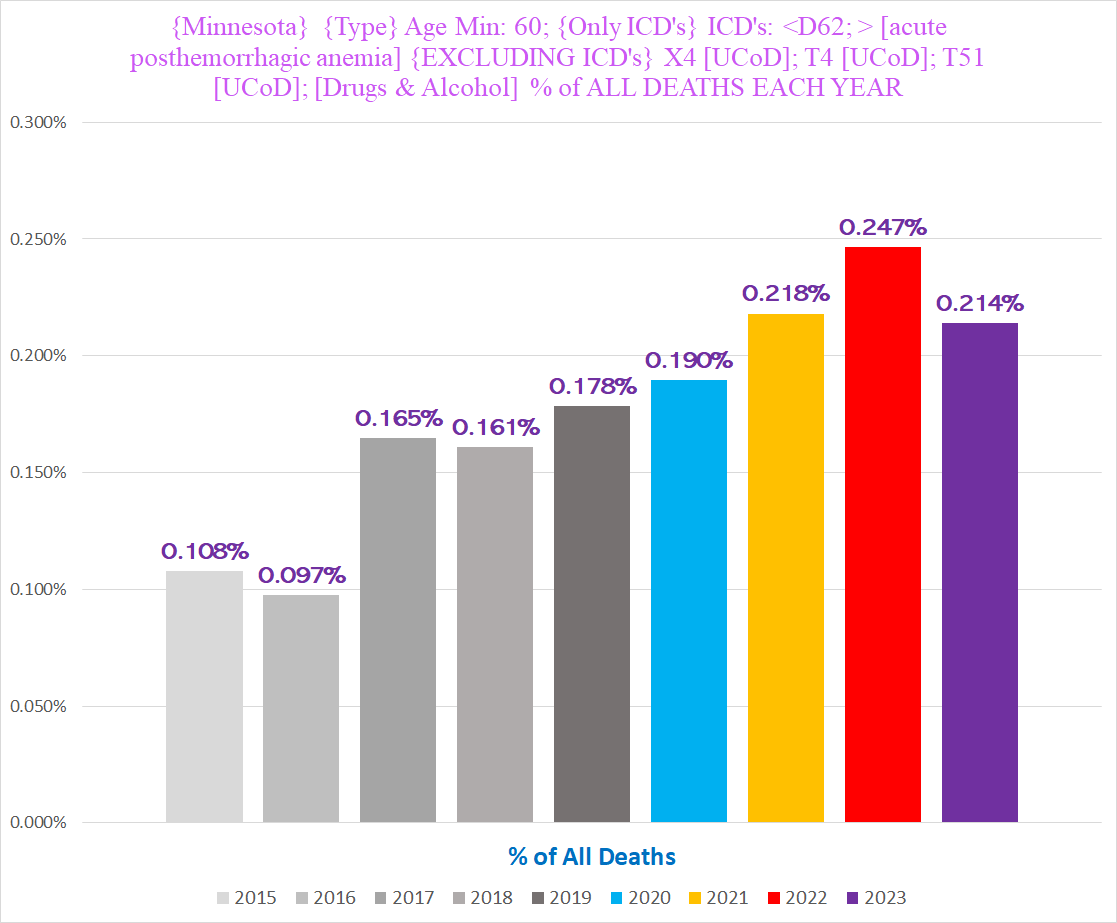
ICD D62 - Acute Posthemorrhagic Anemia
Acute Posthemorrhagic Anemia, or acute blood loss anemia, refers to the depletion of healthy red blood cells with hemoglobin either due to the loss of blood or due to the destruction of red blood cells without blood loss. (For instance, red blood cells will splinter into pieces under sufficient pressure.)
Either way, it is a very dangerous condition to have.
I initially thought that these would feature a large number of accidental deaths involving traumatic injuries with copious blood loss. To my great surprise, I was dead wrong - there were only 13 deaths ruled an ‘accident’ out of 701 APA deaths ages 60+. I went through a bunch of them at random, and they seemed to be mostly either ‘acute blood loss anemia’ with internal bleeding or without further explanation.
The following chart shows the total number of deaths ages 60+ with APA as a CoD:

Here’s the % of all deaths that have APA as a CoD:
There is only one time period where APA and covid align - the winter of 2020/21; the rest of the time APA has no correlation at all:

Here’s the gender breakdown:

So the question remains: why are there excess deaths involving blood loss from internal bleeding?
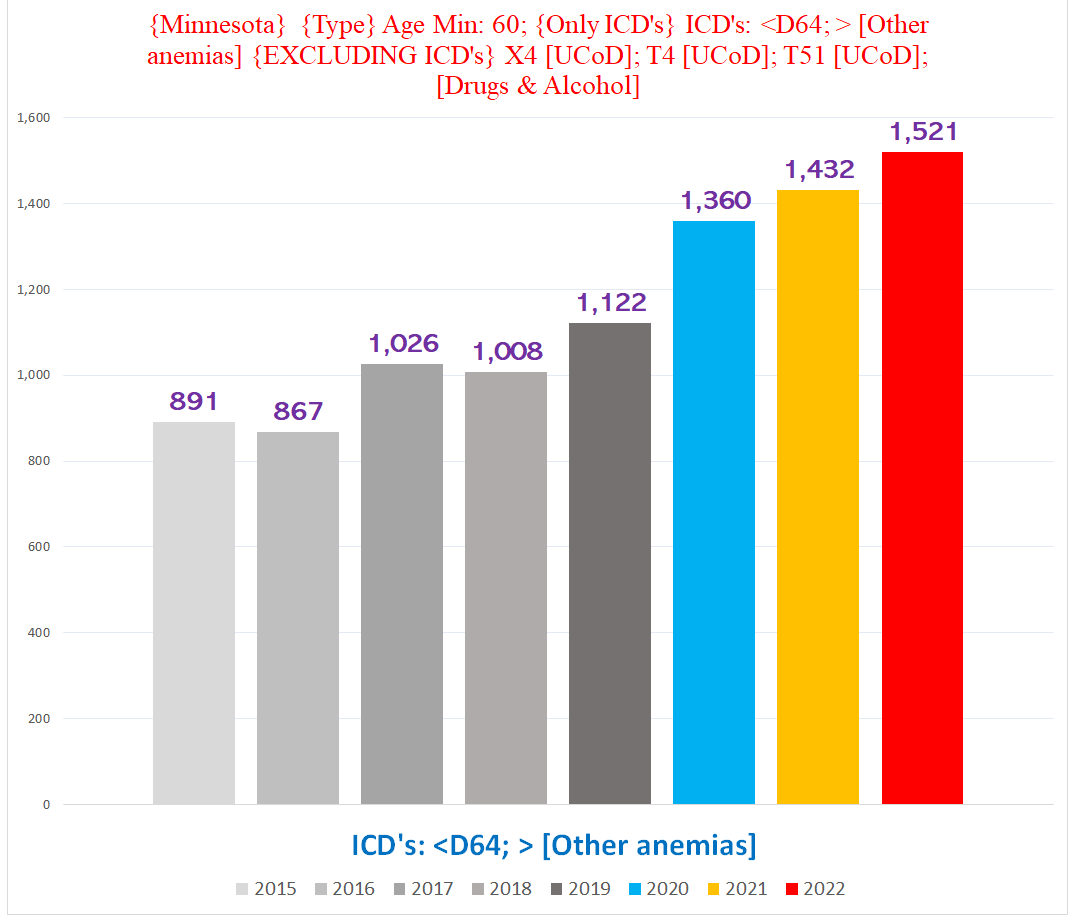
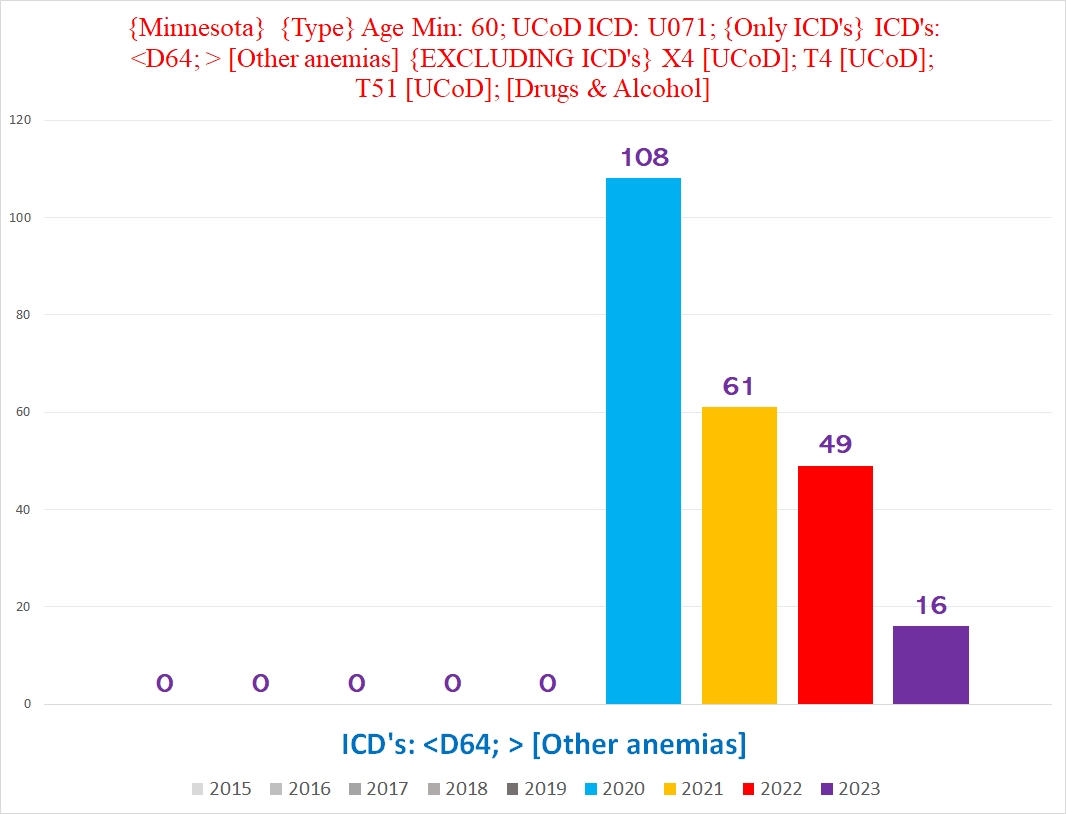
ICD D64 - Other anemias
Based on randomly sampling about 100 of them, D64 is assigned by the CDC to death certificates where the coroner wrote “anemia” without any further explanation (although about 10% had another CoD involving bleeding or hemorrhage of some sort).
In other words, deaths involving an unspecified type of loss or depletion of healthy red blood cells.
Like the previous anemias, D64 is heavily concentrated in older people.
The following chart shows the total number of deaths with ICD Code D64, ages 60+:
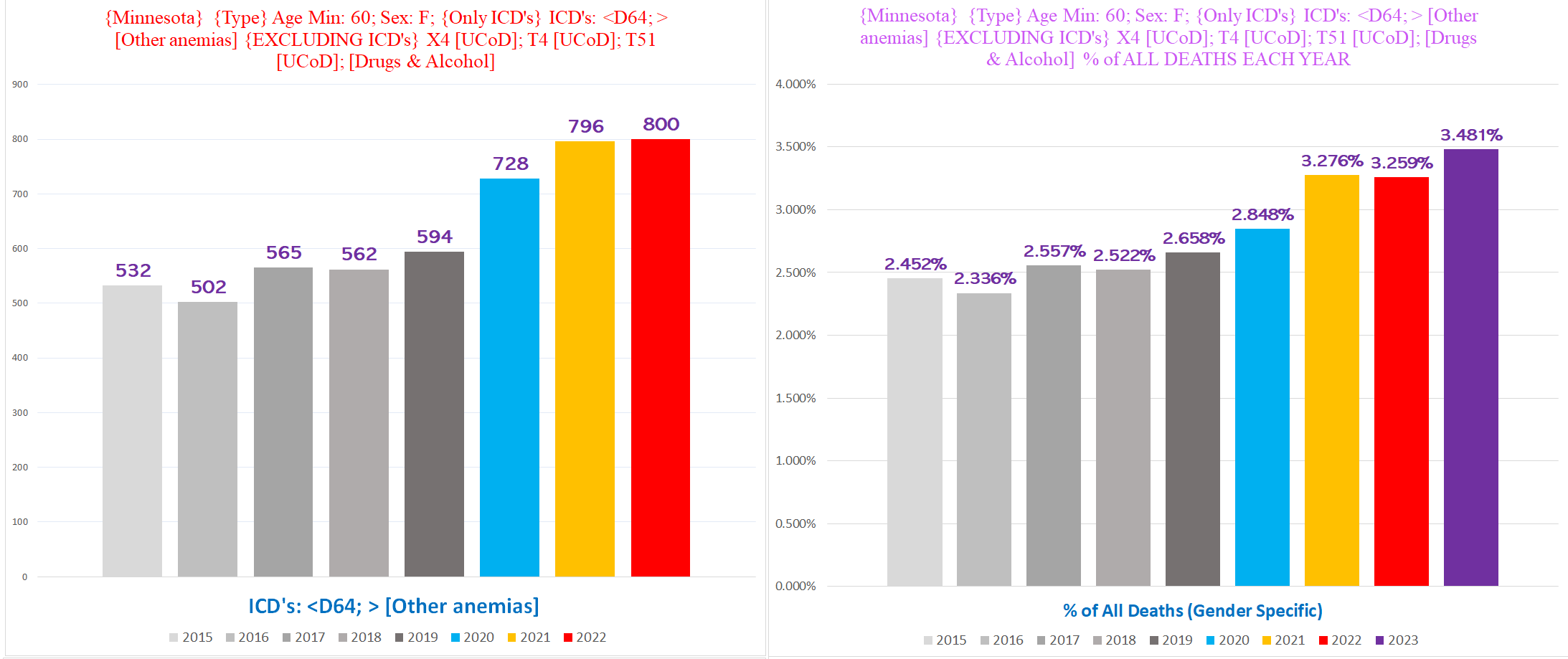
Although there is obvious excess in both genders, the trend is a bit clearer in the women.
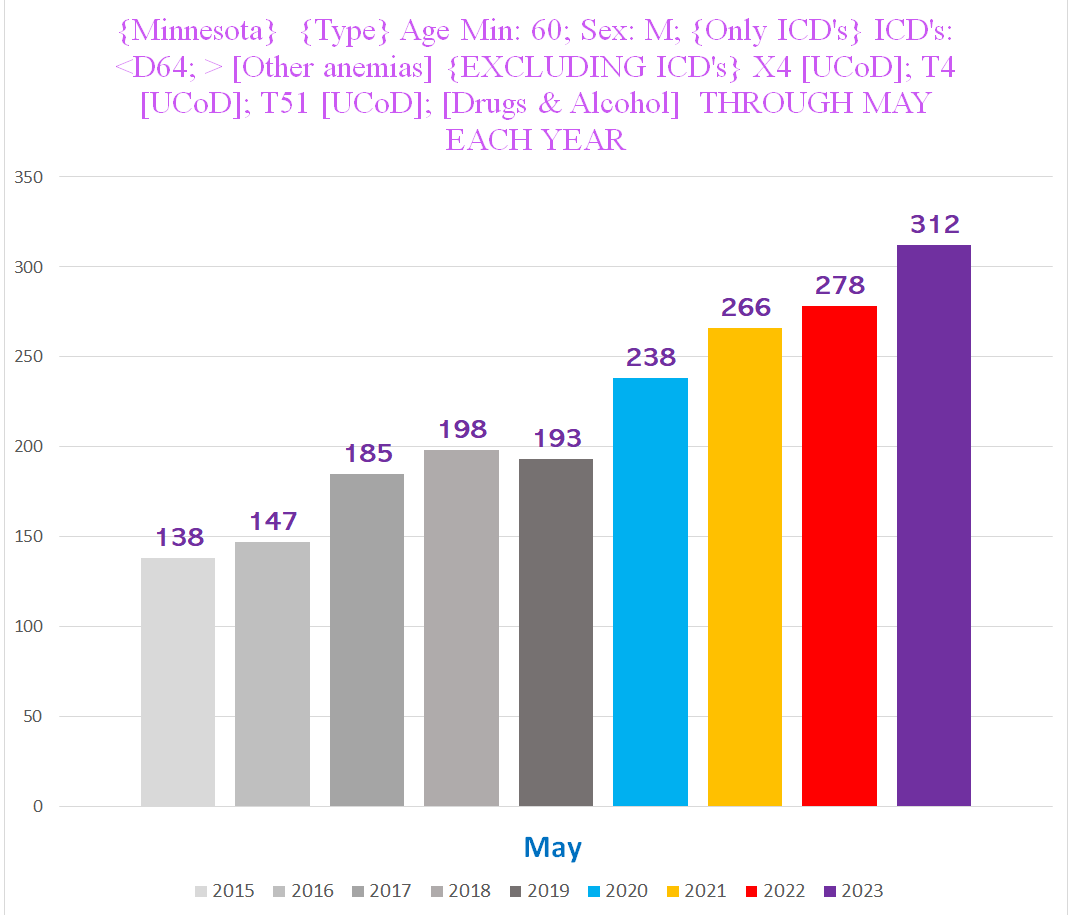
Men:
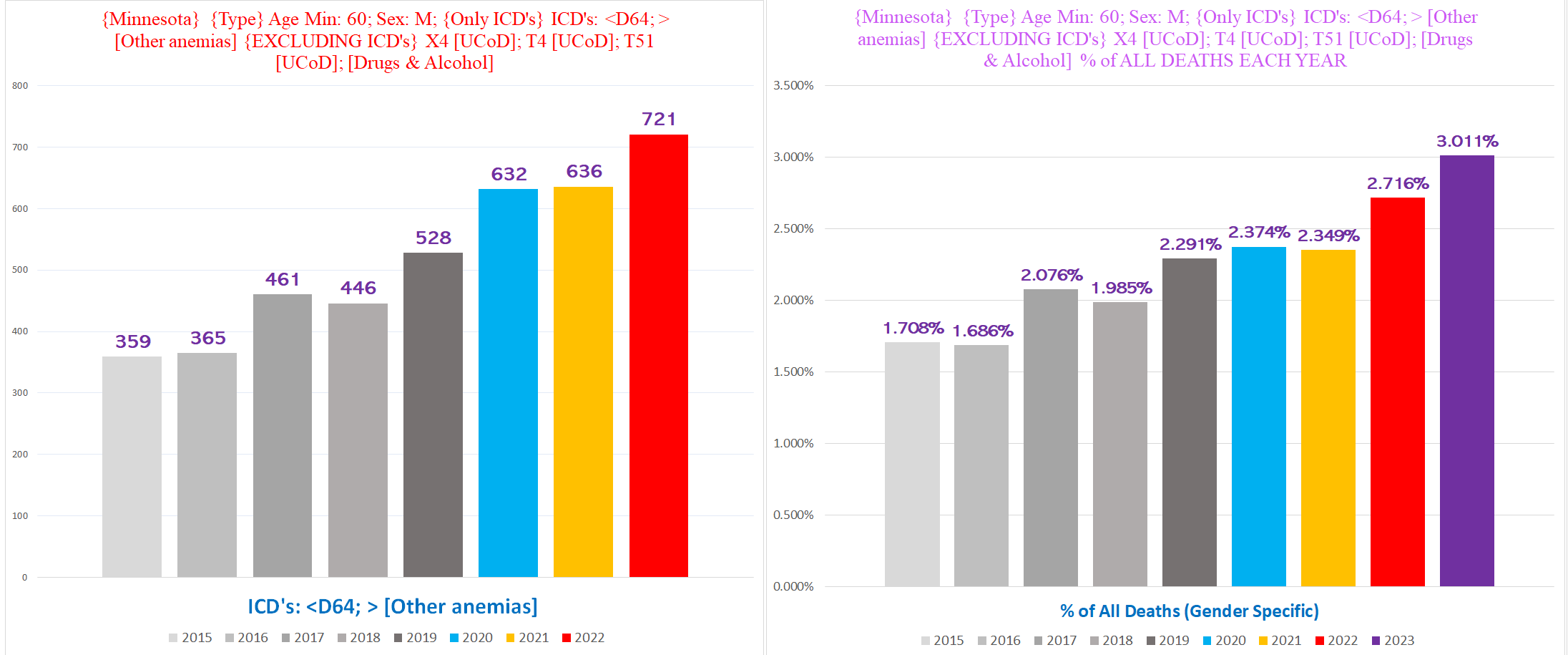
To get an idea of how bad this is getting in the men, here is the total # of Anemia deaths Jan-May each year:
Women:
Unlike the previous anemias, there is a substantial degree of alignment with the incidence of deaths listing covid as a CoD until 2022 when covid flatlines at around 50-100 deaths per week but anemias remain elevated and fluctuating (covid in purple, anemias in red):
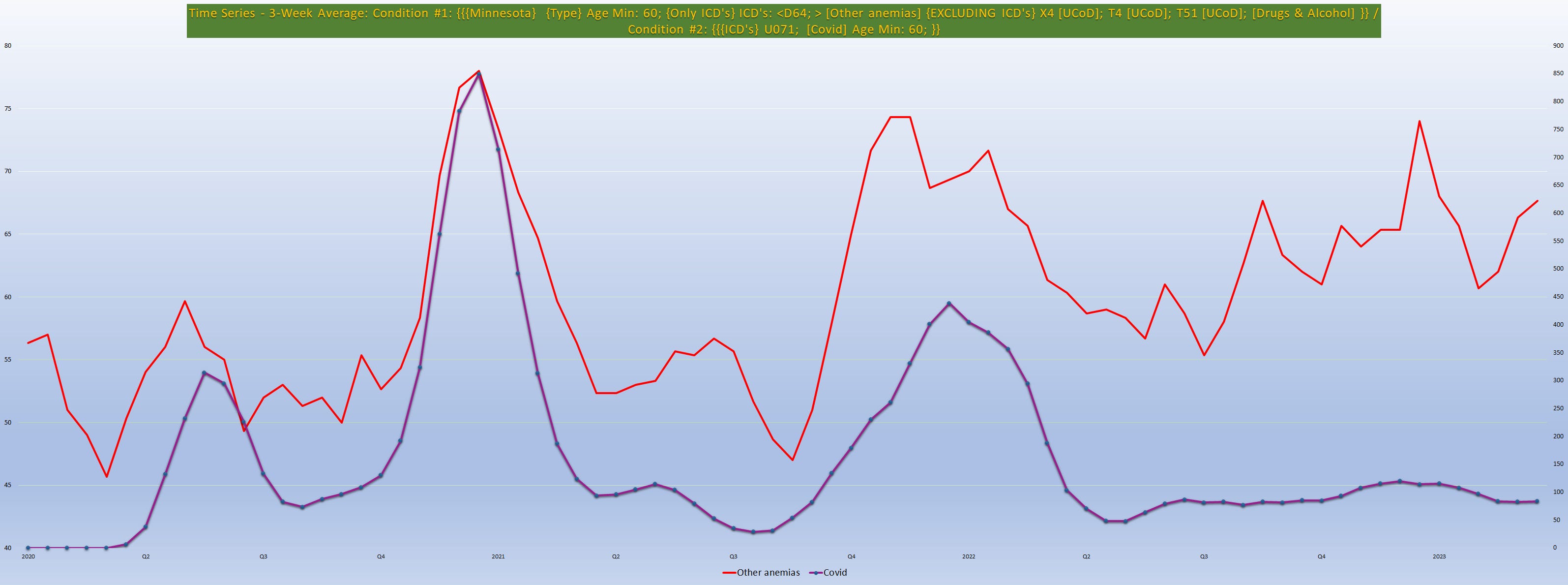
The following chart shows the full time series for anemias layered on top of covid stretching back through 2015 to convey the steady-state excess of anemia deaths from mid 2021-present:

Despite the seeming correlation between anemia and covid deaths, there are very few covid UCoD deaths with anemia, especially after 2020, visualized by the following chart displaying the total number of deaths where covid was the UCoD AND D64 was a listed CoD:
Even if we assume that every single one of these covid-anemia deaths is a genuine covid death, that would only account for about 15-20% of the excess anemia deaths in 2021 & 2022; and <10% of the excess so far in 2023. And this is a tenuous assumption at best.
Ergo, there is clear, non-covid excess of anemia deaths in Minnesota for 2021, 2022 and 2023.
ICD D65 - Disseminated Intravascular Coagulation
According to the NIH, “Disseminated intravascular coagulation (DIC) is a rare but serious condition that causes abnormal blood clotting throughout the body's blood vessels.” Put simply, clotting all over the body.
The following two charts show the total number of male deaths with ICD Code D65 (top) and the % of all male deaths with D65 (bottom):


Fortunately it seems that 2023 is reverting to baseline so far; however, something happened in 2021/2022.
ICD D685 - Primary Thrombophilia
Thrombophilia is where your blood clots too easily, and can be caused by a number of different conditions. Primary or hereditary thrombophilia refers to thrombophilia caused by a genetic mutation in a gene that codes for one of the proteins involved in the clotting process that causes too much of one to be produced, or makes it harder to dissolve the protein after a clot has formed leading to a buildup of little clots that can eventually become a big clot.
The following two charts show the total number of deaths with ICD Code D685 (top) and the % of all deaths with D685 (bottom):
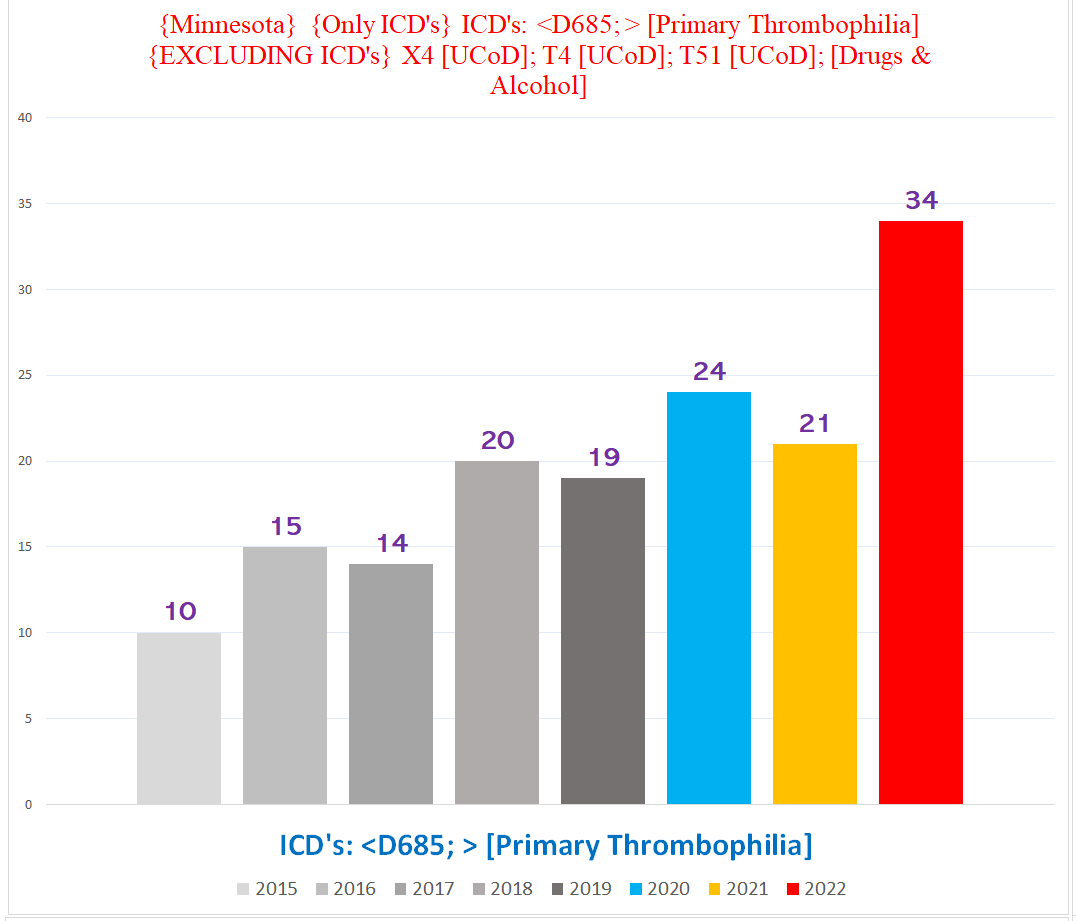

Since this is a genetic condition and the average age of these deaths is well over 70 from 2017 onwards, the likely interpretation of this trend is that people with thrombophilia were at a higher risk of being killed by something else in 2022 & 2023 compared to the general population:

(The spike in the average age in 2020 is entirely due to the 9 deaths in people 90+ years old compared to an average of ONE per year prior to the pandemic, something probably attributable to covid and/or covid policies.)
It seems implausible that covid could be the cause for the excess in 2022, because covid in 2022 is a far milder disease than it was in 2020 or 2021, and only four D685 deaths also had U071 for covid.
ICD D689 - Unspecified Coagulation Defects
This category pretty much refers to what is sounds like - cases where the coroner wrote something like “coagulopathy” or “hypercoagulable state” without providing further details. In other words, unspecified conditions involving too much or too little clotting.
The following chart shows the total number of deaths per year with D689:

It’s hard to know what precisely ‘unspecified’ category conditions represent, because they are by definition cases where the coroner didn’t provide sufficient details. However, in our case, we can presume that they at least represent genuine excess mortality (as opposed to simply being the result of that coroners were lacking information in a higher % of cases), because there are already plenty of excess deaths involving coagulation defects without accounting for the ‘unspecifieds’, so these excess are in addition to the the specified-type coagulation deaths.
I fought anemia for years as a young person. I am now considering how my childhood jabs (1964 onward) may have been related. I did also suffer very very bad nosebleeds from the age of 6-7 years old, much clotting and not stopping. Oh, if we only knew then what I know now. I thought I was just unhealthy, and now I know it's the western medical industry that is horridly murderous and has been since it's inception.
I get blood lab work every 6 months, D is my low-value one. The Endo never says a word about it. As it is integral to bone health he should be. All he is looking at is T3/4 and A1C1 levels. Cardio looks at the Cholesterol levels, and I tell him to Kiss my Grits I'm not taking Statins, in no uncertain terms. My arteries are not blocked. I've had an Enlarged Heart for a long time no doctor has ever said a word about with a small Mitral Valve leak until I saw an Asian neurologist for Neuropathy leg swelling. Strange at 60 she found it with just a stethoscope. It is a family genetic thing.