


Dr. Berman on Vaccine vs Natural Immunity
Claim: “For those with natural immunity, whether or not to get vaccinated is for another discussion.”

This is part of a series to highlight the ineptitude and sheer illiteracy of the experts my community has relied upon for covid medical advice. I am only employing arguments that can be made from the data/studies and other information available at the time the claim was made.
Claim: “For those with natural immunity, whether or not to get vaccinated is for another discussion.”
Source: On the Covid Vaccinations, published 6/21/21
Background: Widespread establishment opinion was that natural immunity is unreliable and inadequate. (To his credit, Dr. Berman did acknowledge that natural immunity had been effective to that point.)
The Facts:
Immunity acquired from covid infection has been demonstrated to be strong, durable, long-lasting, and effective for all variants.
Every comparison between infection immunity and vaccine immunity at the time showed infection immunity to be superior.
There was not then, nor has there ever been, any basis to doubt infection immunity.
There was already evidence then that vaccine immunity might be weak against already circulating variants.
There was already evidence that the vaccines, especially the 2nd dose, can weaken prior immunity from infection.
Although Dr. Berman did not affirmatively endorse previously infected individuals getting vaccinated, his espousal of vagueness is itself markedly inconsistent with the available clinical evidence.
Studies such as:
Covid-19 immunity likely lasts for years | MIT Technology Review
Lasting immunity found after recovery from COVID-19 | National Institutes of Health (NIH)
SARS-CoV-2-specific T cell immunity in cases of COVID-19 and SARS; and uninfected controls
SARS-CoV-2 infection induces long-lived bone marrow plasma cells in humans;
Exposure to SARS-CoV-2 generates T-cell memory in the absence of a detectable viral infection
have all found that natural immunity induced by infection running the gamut of severity including asymptomatic exposure is extremely robust, durable, and/or sharing bio-markers with the immunity induced by the 1918 Spanish Influenza (Neutralizing antibodies derived from the B cells of 1918 influenza pandemic survivors found remained active after 100+ years) and SARS-CoV-1 (SARS-CoV-2-specific T cell immunity in cases of COVID-19 and SARS, and uninfected controls found still currently present in infected individuals nearly 20 years later).
Assessment of protection against reinfection with SARS-CoV-2 among 4 million PCR-tested individuals in Denmark in 2020: a population-level observational study found a 0.65% reinfection rate compared to 3.27% for uninfected individuals, a reduction >80%. SARS-CoV-2 antibody-positivity protects against reinfection for at least seven months with 95% efficacy describes its findings in the title.
This finding is bolstered by the similarly substantially documented cross-reactivity of other immunities to SARS-CoV-2, such as:
Targets of T Cell Responses to SARS-CoV-2 Coronavirus in Humans with COVID-19 Disease and Unexposed Individuals - which reported “we detected SARS-CoV-2-reactive CD4+ T cells in 40%–60% of unexposed individuals, suggesting cross-reactive T cell recognition between circulating ‘‘common cold’’ coronaviruses and SARS-CoV-2”;
and
Presence of SARS-CoV-2-reactive T cells in COVID-19 patients and healthy donors, who reported “[w]e demonstrate the presence of S-reactive CD4+ T cells in 83% of COVID-19 patients, as well as in 34% of SARS-CoV-2 seronegative healthy donors (HD) […]”.
(Cross-reactive immunity is a long-established phenomenon going back decades easily discovered by means of a simple Google search, and also documented for, off the top of my head, H1N1, Seasonal H1N1 Influenza Virus Infection Induces Cross-Protective Pandemic H1N1 Virus Immunity through a CD8-Independent, B Cell-Dependent Mechanism).
Furthermore, practically every study that compared natural immunity and vaccination immunity found natural immunity to be superior (the slim minority that found otherwise all did so on the basis of surrogate bio-markers never proven to correlate with immunological outcomes, and refuted by ubiquitous real-world observation):
Pfizer’s massive study surveying almost the entire Israeli population, Protection of previous SARS-CoV-2 infection is similar to that of BNT162b2 vaccine protection: A three-month nationwide experience from Israel, found that natural immunity was slightly more effective than their vaccine’s immunity.
A recent Cleveland Clinic study likewise found that while there were a few breakthrough cases of covid amongst their vaccinated employees, the natural immunity among unvaccinated employees was a perfect 100% impervious(!), leading the study’s authors to conclude “Individuals who have had SARS-CoV-2 infection are unlikely to benefit from COVID-19 vaccination” (which, translated from the typically restrained parlance of academia, means that they couldn’t fathom any plausible justification to vaccinate PI’s).
Single cell profiling of T and B cell repertoires following SARS-CoV-2 mRNA vaccine found that “[n]atural infection induced expansion of larger CD8 T cell clones occupied distinct clusters, likely due to the recognition of a broader set of viral epitopes presented by the virus not seen in the mRNA vaccine”.
Recent data from Israel where vaccinated people were almost 7x as likely to be infected as recovered individuals likewise suggests the superiority of infection induced immunity to its vaccine counterpart.
Natural immunity has further been demonstrated superior to vaccine induced immunity regarding variants. At that time, there had not been any legitimate study that found natural immunity’s neutralization capacity suspect for any variant, versus a few that specifically found the protection of natural immunity against variants to be robust, such as:
Identification of SARS-CoV-2 Nucleocapsid and Spike T-Cell Epitopes for Assessing T-Cell Immunity
SARS-CoV-2–specific CD8+ T cell responses in convalescent COVID-19 individuals
The NIH itself even issued a statement confirming the obvious: T cells recognize recent SARS-CoV-2 variants.
In sum, the worldwide incapability to document genuine reinfection phenomena in significant numbers (how many nursing homes have you heard about experiencing multiple covid outbreaks months apart?) despite the emergence of numerous ‘variants of concern’ foreclosed rational skepticism regarding natural immunity’s potency repelling covid variants.
Neutralization capacity of vaccine immunity, on the other hand, presents obstruse ambiguity in light of recent studies such as Multiple SARS-CoV-2 variants escape neutralization by vaccine-induced humoral immunity and Live virus neutralisation testing in convalescent patients and subjects vaccinated against 19A, 20B, 20I/501Y.V1 and 20H/501Y.V2 isolates of SARS-CoV-2, which cast serious doubts on the viability of vaccine immunity to hold up against emerging variants (something that has since been proven to be a well-founded concern.
(There were other studies, but I was unsuccessful in quickly locating them when I first wrote this, which was around the time that Dr. Berman’s article was published.)
The superiority of natural immunity is anyway a practically tautological proposition, simply because whereas the induced immunity of the vaccines employing a gene therapy mechanism is limited to epitopes of the spike protein in its prefusion state, natural immunity develops antigen-specific immune cells to most if not all epitopes of the covid virion from all stages of viral activity, which studies such as T cell Epitopes: adaptive immune response against COVID-19 have found to number well over a thousand.
Furthermore, studies such as Immunity after SARS-CoV-2 infections, published in Nature Immunology, found that the non-Spike protein epitopes accounted for a majority of SARS-CoV-2 antigen-specific T-Cells in previously infected subjects, and suggested enhancing the vaccines by broadening the targeted epitopes beyond specific S-protein ectodomains.
Unbiased Screens Show CD8+ T Cells of COVID-19 Patients Recognize Shared Epitopes in SARS-CoV-2 that Largely Reside outside the Spike Protein summed up their findings thusly:
In total, we identified 3–8 epitopes for each of the 6 most prevalent human leukocyte antigen (HLA) types. These epitopes were broadly shared across patients and located in regions of the virus that are not subject to mutational variation. Notably, only 3 of the 29 shared epitopes were located in the spike protein, whereas most epitopes were located in ORF1ab or the nucleocapsid protein. We also found that CD8+ T cells generally do not cross-react with epitopes in the four seasonal coronaviruses that cause the common cold. Overall, these findings can inform development of next-generation vaccines that better recapitulate natural CD8+ T cell immunity to SARS-CoV-2.
This echoes simple timeless wisdom embodied in modest aphorisms such as “don’t put all your eggs in one basket” that ought inform clinical judgement that immunological memory which catalogues all epitopes of a pathogen surely is preferable to immunity restricted to a limited number of epitopes, all native to one protein. (The indignant howls of vaccine proponents that the spike protein’s uniquely potent immunogenicity more than adequately compensates for the vaccine’s narrow targeting are merely that, and not particularly accurate besides.) Covid infection furthermore engages the entirety of the immune system naturally, which is presumptively catalyzing the peak robust, healthy and balanced priming of the immune system, which cannot be said for a vaccine whose mechanism is a marked deviation from the manner in which natural infection engages the immune system.
Regarding mass-vaccination in general, Impact of Influenza Vaccination on Seasonal Mortality in the US Elderly Population found rather startlingly that:
“We could not correlate increasing vaccination coverage after 1980 with declining mortality rates in any age group. Because fewer than 10% of all winter deaths were attributable to influenza in any season, we conclude that observational studies substantially overestimate vaccination benefit.”
This suggests at minimum that the scientific community has a distorted sense of the utility of mass vaccination campaigns.
A comprehensive UK report on ‘variants of concern’, SARS-CoV-2 variants of concern and variants under investigation in England, discovered that the death rate from the Delta variant among fully vaccinated was more than 6x the rate among the unvaccinated (26/4087 vs 34/35,521):
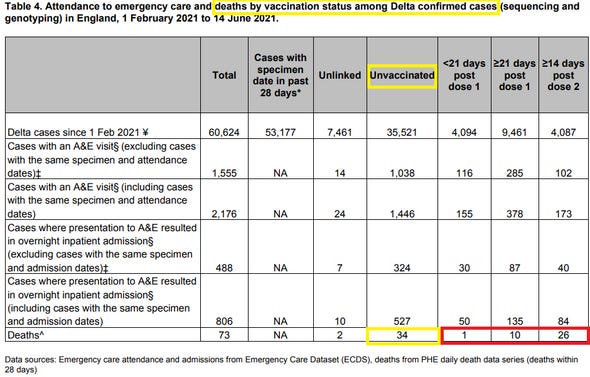
(Yes, this is far from clear cut, and there are numerous confounding factors in play. However, the medical community’s pattern of willful blissful ignorance of possibly embarrassing raw data with potential implications at odds with their favored positions and promulgations is demonstrative of rampant intellectual dishonesty by policy makers and their medical advisors.)
The primary consideration that militates unabashedly against vaccinating previously infected persons is that there exists evidence that vaccines can “exert a detrimental effect” upon the already existing immunity from prior covid infection. As reported by Differential effects of the second SARS-CoV-2 mRNA vaccine dose on T cell immunity in naïve and COVID-19 recovered individuals,
“the second vaccination dose appears to exert a detrimental effect in the overall magnitude of the spike-specific humoral response in COVID-19 recovered individuals”, and “the second BNT162b2 vaccine dose results in a reduction of cellular immunity in COVID-19 recovered individuals, which suggests that a second dose, according to the current standard regimen of vaccination, may be not necessary in individuals previously infected with SARS-CoV-2.”
(Random observation – the authors assertion that “that a second dose, according to the current standard regimen of vaccination, may be not necessary in individuals previously infected with SARS-CoV-2” is bizarre – the rational conclusion from their finding isn’t that the 2nd dose ‘may not be necessary’, rather it is ‘the 2nd dose for already infected persons must be precluded for that entire population’ (at least until further research can assess the immunological impact of the 2nd dose).)
Moreover, studies such as Self-reported real-world safety and reactogenicity of COVID-19 vaccines: An international vaccine-recipient survey and Previous COVID-19 infection but not Long-COVID is associated with increased adverse events following BNT162b2/Pfizer vaccination found that the risks of adverse effects is potentially greater by orders of magnitude for non-naïve individuals. Besides, there are no studies or reports derived from real-world observation suggesting that vaccination enhances natural immunity in any setting. (The CDC attempted to simply lie about this and was caught by Congressman Thomas Massie.)
In conclusion, employing Dr. Berman’s own articulated standard requiring provision of demonstrable basis undergirding any speculation, one cannot conceivably doubt the immunity engendered by natural infection, whereas the immunity profile of the currently available covid vaccines still contains significant unresolved ambiguity. Taken concomitantly with the already-identified potential reductive impact of vaccination on prior immunity and considerably heightened risks of adverse effects, this presents an unrebuttable case that vaccinating previously infected individuals lacks discernable clinical benefit, and is an immoral violation of foundational medical ethics resolved in Nuremberg and Helsinki.