


Dr. Berman on Vaccinating Children
Claim: The risk/benefit analysis of the covid vaccines clearly favors vaccinating children.

This is part of a series to highlight the ineptitude and sheer illiteracy of the experts my community has relied upon for covid medical advice. I am only employing arguments that can be made from the data/studies and other information available at the time the claim was made.
Claim: The risk/benefit analysis of the covid vaccines clearly favors vaccinating children.
Source: On the Covid Vaccinations, published 6/21/21
Background: Most of the data on vaccine injuries in kids, especially myocarditis, was not available at the time.
The Facts:
Kids without severe covid risk factors are not at risk for serious covid-caused problems.
Kids are at risk from the vaccines far more than from covid itself.
Since kids don’t spread covid in meaningful numbers, vaccinating kids is unlikely to have a significant effect in reducing transmission.
Vaccines might have a negative impact on kids naturally amazing immunity to covid.
Despite the absurd apologetic contretemps of the CDC, children younger than 18 face considerably greater threat of illness and severe adverse incidents from the vaccines than from covid itself. Notably, almost every alleged pediatric covid death befell children with severe comorbidities, and that’s without controlling for overcounted pediatric deaths due to hyper-aggressive COD coding policies implemented throughout the US and the world. The CDC themselves recently acknowledged (at the time) this was occurring in a MMWR report, mmwr/volumes/7 (the report represents the absolute minimum % of covid deaths misattributed to covid, not the ceiling):

(It is worth emphasizing that the CDC discovered 39 ‘self-inflicted deaths’ and 13 homicides (for the record, a significant undercount) somehow attributed to covid, plainly exhibiting the remarkable extent of political entanglement with clinical judgement, whereby political considerations superseded elementary judgement so much so that coroners engaged in blatant fraud whose deceit was self-evident to even the common layperson.)
Additional evidence demonstrating the negligible covid mortality borne by the pediatric demographic comes from a study published in the Lancet, a portion of it reproduced below:
Since early reports from China stated that severe COVID-19 disease was rare in children, we have analyzed child COVID-19 mortality in seven countries. To put the deaths into a context that would help the understanding of parents, clinicians, and policy makers, we previously made comparisons of COVID-19 deaths with modelled mortality from all causes and other causes. Our first publication in April, 2020, was followed by a trend analysis up to August, 2020. We also update a data table online. Here, we update this analysis to February, 2021, in light of increases in adult mortality through the 2020–21 winter, and concerns about variant B.1.1.7, first identified in the UK in December, 2020 (probably circulating since September).
Table of Age-specific data for seven countries showing estimated all-cause deaths compared with COVID-19 deaths:
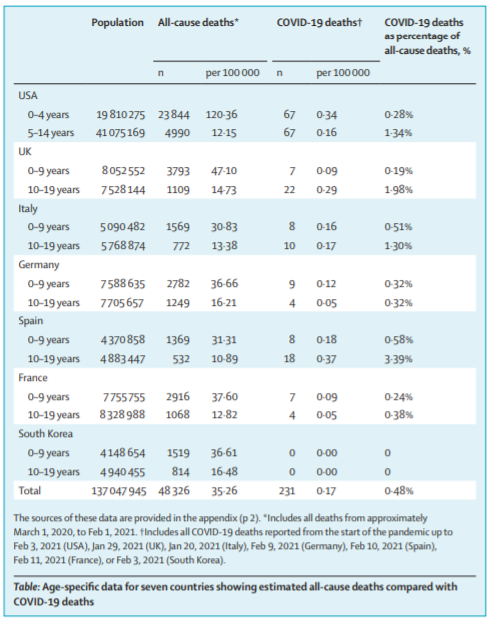
The sources of these data are provided in the appendix (p 2).
* Includes all deaths from approximately March 1, 2020, to Feb 1, 2021.
† Includes all COVID-19 deaths reported from the start of the pandemic up to Feb 3, 2021 (USA), Jan 29, 2021 (UK), Jan 20, 2021 (Italy), Feb 9, 2021 (Germany), Feb 10, 2021 (Spain), Feb 11, 2021 (France), or Feb 3, 2021 (South Korea).
(I used the table from the PDF version, which is why you won’t find the source †/*.)
This sort of politicized bureaucratic malfeasance has similarly contaminated all of the other covid metrics. The hospitalization data for pediatrics (and for everyone else to a vaguely lesser extent) is riddled with the same rank incompetence/malevolence.
The Public Health Agency of Canada recently published a report that found “only 36.6% of pediatric patients hospitalized with COVID-19 were admitted due to an acute respiratory infection”.
This is in line with recent studies in the US that similarly found an estimated 45% of pediatric hospitalizations to be incidental positives in patients admitted for wholly unrelated reasons (although I suppose that admittance for a gunshot whose lethal pathology is attributable to covid upon death can be reasonably categorized as a hospitalization because of covid).
Long Covid
One of the most enduring and pernicious deceptions promulgated regarding pediatrics is that there is that children, including healthy children, are susceptible at a statistically significant rate to the poorly defined, dreaded ‘long covid’. This is, firstly, yet another form a long line of unwarranted and reckless assumptions by the medical community devoid of any evidentiary basis that can exclude other causes or places the rate of children presenting any of over 200 symptoms (!!!) significantly higher for documented covid infections than for those without covid infection. Secondly, research attempting to assess these characteristics has found that there is not a documentable phenomenon of children suffering from long covid. Vaccinating children to prevent long covid? More caution is needed in interpreting current epidemiological data, published in the BMJ, declared:
The ONS figures6 need context. Our understanding is that they represent the proportion of children who—within five weeks of a positive covid-19 test—have one of the following symptoms: fatigue, cough, headache, loss of taste or smell, myalgia, sore throat, fever, shortness of breath, nausea or vomiting, diarrhea, or abdominal pain. For some of these symptoms the ONS reported prevalence is as follows: fatigue 3.5%; cough 4%; headache 5.3%; loss of taste or smell 2%; myalgia 1.7%. These seem in line with or lower than the population prevalence—for example, cough reported in an unselected cohort of 7670 children aged 1-18,7 or headache and fatigue in children from a representative Finnish cohort.8 Given current high levels of family and community stress we would expect the prevalence of some of these symptoms to be higher.
The prevalence estimates being discussed need a comparator group, and to be interpreted with much more caution, especially given the lack of a dedicated case definition for children.9 Specifically, we need to know how many survey participants (by age) without covid-19 had similar symptoms. In the meantime—especially while there are no safety data in children—we endorse the Royal College of Paediatrics and Child Health’s sensible position on covid-19 vaccination.10
Long-term symptoms after SARS-CoV-2 infection in school children: population-based cohort with 6-months follow-up, found that:
“[s]eropositive children, all with a history of pauci-symptomatic SARS-CoV-2 infection, did not report long COVID more frequently than seronegative children. This study suggests a very low prevalence of long COVID in a randomly selected population-based cohort of children followed over 6 months after serological testing.”
And to cap it off, even the CDC hasn’t officially declared there to be a causal link (or any link at all) between MIS-C (one of the primary alleged ‘long covid’ outcomes) and covid. From the CDC website:
On the other hand, the Canadian study Environmental epidemiology of Kawasaki disease: Linking disease etiology, pathogenesis and global distribution found about Kawasaki (functionally renamed MIS/-C last year) that:
“Patients with KD were generally less exposed to environmental allergens in many aspects of their daily lives (Table 3). They were more likely to primarily drink filtered or bottle water, were exposed less to household pets, were more likely to live in a dwelling constructed in the last 10 years and were less likely to live in an area with dense tree coverage, near a park, body of water or a farm. There was some statistically significant associations between the different exposures reported in Table 3.”
In other words, Kawasaki/MIS-C is more likely to occur in the absence of exposure to natural allergens and pathogens… a likely byproduct of lockdowns. Whoops.
Furthermore, there has not yet been any attempt as far as I’m aware of to quantify the epidemiological impacts of the covid policies on the individual health of populations, such as prolonged wearing of facemasks, lockdowns, social isolation, diet, exercise, and various markers of health, among other factors. Simply claiming that any adverse conditions found in anyone without a clear or observable cause is attributable to covid is rank negligence unbefitting a college student, much less amply credentialed medical practitioners and health experts.
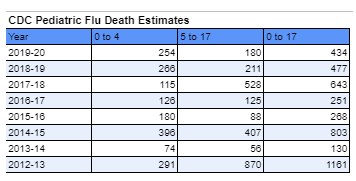
The flu/influenza, by comparison, imperils children with considerably graver morbidity and mortality risks compared to covid, including ‘long Flu’, from the routine seasonal flu/influenzas:
On the flip side, the outsized quantity and severity of pediatric adverse health events post-vaccination is a phenomenon widely documented, from both pediatric vaccine trial data and from subsequent real-world deployment. The following table shows the frequency of systemic side effects to children in the Pfizer pediatric vaccine trial, and it is not a pretty sight:
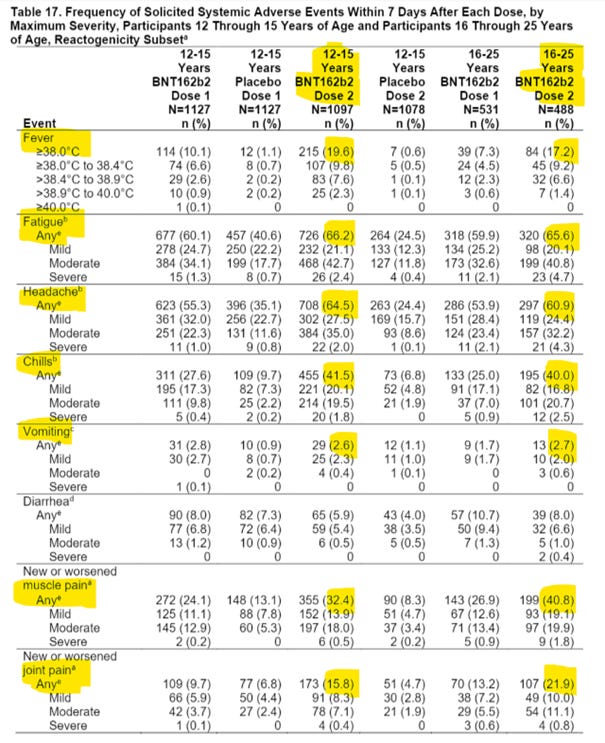
Remember, per the actual trial, this prevented a mere 30 MILD COVID CASES.
Then there are the Serious Adverse Events (SAE’s). Even per Pfizer's own trial data (p. 27), from just one month of observation, there is an approximately 1-in-330 risk for a serious adverse event (SEA) from the vaccines (5/1,127 12- to 15-year-olds in the vaccine group, vs 1/1,127 of the placebo group).
Israeli data on the Pfizer vaccine for adults published in the New England Journal of Medicine (p.22) found that the "needed to treat" # per life saved is 27,778 (19 fewer deaths/vaccine group vs placebo group, out of 526,877 people = 1/0.00036 = 27,778).
This indicates that the ‘need to treat #’ as applied to children is stratospherically higher, because as a significant majority of the population already possesses immunity of whatever provenance (infection, cross-reactive, and/or vaccine), the epidemiological impact of each additional vaccinated individual is greatly reduced. This trait is especially pronounced in children, whose proven disposition as non-vectors severely diminishes their baseline individual forward-transmitting capability.
Furthermore, the NTT# to clinically benefit healthy children is comically colossal simply because there is literally almost no documented covid deaths in the healthy pediatric demographic. Again, this is using Pfizer’s own data (which I would strongly contest and is possibly a topic for a future essay).
Further recent research such as Shared B cell memory to coronaviruses and other pathogens varies in human age groups and tissues indicates that children possess uniquely potent cross-reactive immunity from common-cold CoV’s, further cautioning against potentially adversely interfering with their amazing innate immunity with vaccines lacking a comprehensive immunological profile (as indicated by the myriad ongoing vaccine trials attempting to flesh this out).
A wholesome look at the broad mosaic of data regarding pediatric immunity plainly stresses that prior mediated immunities of any provenance is palpably and vigorously manifest in the statistically negligible disease burden carried by the pediatric demographic. This combined with the definite risks of vaccine SAE’s already visible, the wholly uncharted vistas of these vaccine’s long-term impacts, and recent research signaling potential hobbling of prior covid immunity by the vaccines, emphatically discourages vaccination of any children. (Vaccinating children uniquely susceptible to covid is another matter that requires further elucidation, although there are plenty of treatments that work on these kids that are safer than the vaccines.)
This is all in addition to the macro- level arguments against mass vaccination spelled out in Dr. Berman on Vaccinating to Herd Immunity.
So no, there is no basis for vaccinating children whatsoever, and the risk/benefit is basically entirely risk and no clinical benefit.