


Debunking JOWMA's Latest Brazenly False Ad About Covid and Children, Part 1
These are indeed "fast facts", as in "fast and loose"

Dr. Eric Rubin, member of the FDA's advisory committee on vaccines and editor of the New England Journal of Medicine, said during the Oct. 26 meeting: "We're never going to learn about how safe the vaccine is unless we start giving it, and that's just the way it goes."
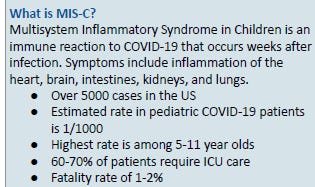
This is the newest delusional fearmongering propaganda proffered by the esteemed medical ‘experts’ at JOWMA:
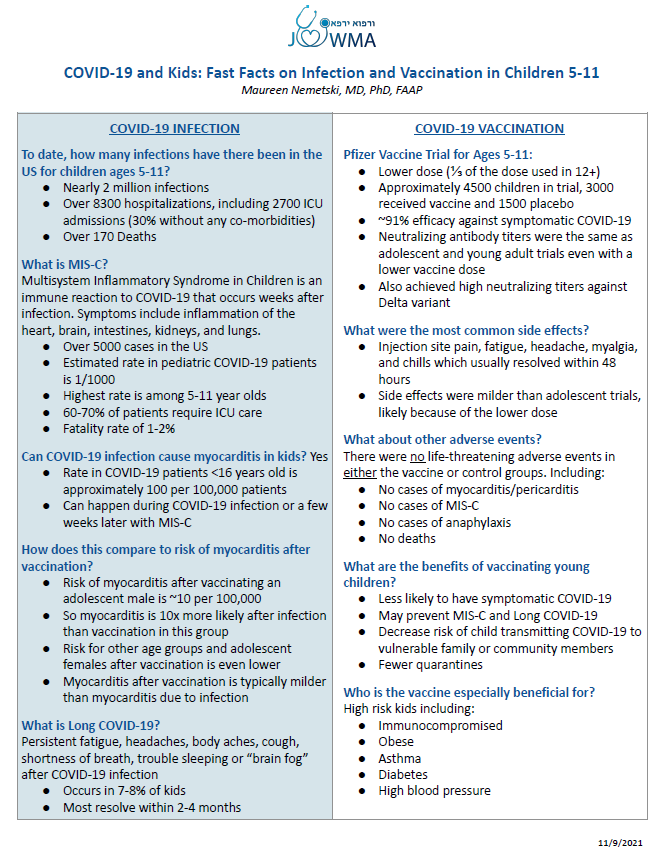
This is so obviously disconnected from reality that it basically refutes itself, because people can see for themselves that healthy kids simply do not get severely ill from covid. However, to our misfortune, the misconceptions carried by many people are similarly disconnected from reality, and most people are not sufficiently literate in the granular data and studies to refute the specific claims made here, so this is worth rebutting in full.
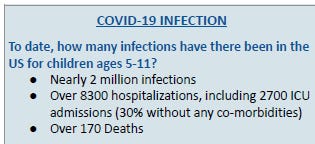
Hmmm, let’s see:
45% of pediatric hospitalizations in the count were unlikely admitted for COVID: “For COVID” or “With COVID”: Classification of SARS-CoV-2 Hospitalizations in Children
At least 40% of covid hospitalizations in kids incidental and another 47% only mildly symptomatic. Characteristics of Hospitalized Children Positive for SARS-CoV-2: Experience of a Large Center
A study published in the Journal of American Academy of Pediatrics found, "Nearly one-half of the infected children had coinfection with other common respiratory pathogens.": Coinfection and Other Clinical Characteristics of COVID-19 in Children
61% of the reported pediatric COVID deaths were not caused by covid: Deaths in Children and Young People in England following SARS-CoV-2 infection during the first pandemic year: a national study using linked mandatory child death reporting data
Compare Dr. Nemetzki’s frightening portrayal to the following courtesy of the CDC:
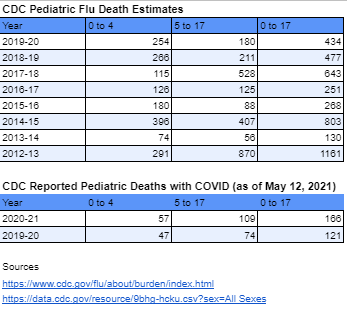
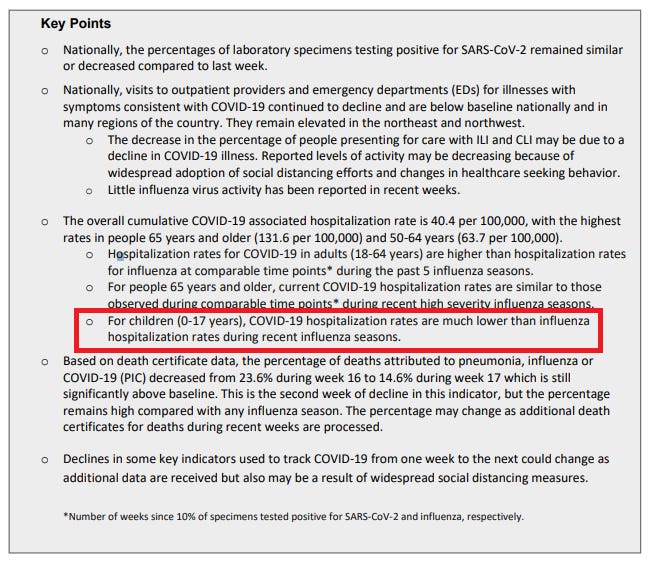
Even the CDC once upon a time openly admitted (page 2) that covid was far less threatening to kiddies than the seasonal Flu/Influenza:
Clearly, not something to play roulette with uncertain vaccine products that have obvious and compelling safety issues (more on this in Part 2).
The following is mostly borrowed from Emily Burns (with some additions and changes):
Even per the CDC’s absurd standards, from March 2020 through now, there have been only 335 pediatric deaths with COVID-19 in the United States. That’s .0004% of the country’s 74 million children age 0-17, and 0.6% of all 49,725 pediatric deaths that have occurred in the same timeframe. Only 65 (19%) of deaths involved pneumonia - which in countries like Singapore is standard for counting all COVID deaths.
CDC case demographic data shows nearly 3.5 million positive COVID tests among age 0-17, which gives us a .0097% case fatality ratio (CFR). “Cases” — which are positive tests, versus actually-sick kids — reflect detected infections, versus all infections.
The agency’s disease burden estimates put the number of infections for children at nearly 27 million between February 2020 - March 2021. By now, we’re at 30 million plus, using “CDC math”. The reality is that by now, more than 50 million kids have had covid.
Regarding the CDC’s absurdly expansive definitions for covid metrics, data from the U.S. and England, respectively, show 35% and 60% of pediatric deaths with COVID-19 were not attributable to the virus. In other words, the death totals include children with other severe conditions or adverse events who tested positive for a virus that didn’t play a part in their deaths. Per a November 2020 study from FAIR Health, among COVID patients with no co-morbidities, age 0-18 had 0.00% mortality (no deaths), compared to 0.01 percent mortality in the same age group among all patients.
The CDC’s pediatric flu death estimates over the past ten years show rates per 100,000 from 0.25 to 1.16 or higher, depending on age. Compare to 0.20 and lower for COVID-19 (not accounting for a potential 35% over-ascertainment, which Phil Kerpen illustrates here).
The CDC’s mid-range estimate for pediatric COVID hospitalizations since February 2020 is ~200,000. HHS data show ~47,000 COVID-positive pediatric admissions since January 2020, with some states reporting only from July 2020 onward. Assuming 27 million infections, that’s a .07% rate. But there’s a catch.
Neither HHS nor CDC data distinguishes between being hospitalized for COVID per se, and being in the hospital for another reason but testing positive incidentally upon admission or during one’s stay. As Marty Makary said in a recent WSJ op-ed, “[The CDC’s] Covid adolescent hospitalization report, like its death count, doesn’t distinguish on the website whether a child is hospitalized for Covid or with Covid…An asymptomatic child who tests positive after being injured in a bicycle accident would be counted as a ‘Covid hospitalization.’”
He’s right. One recent study at a children’s hospital in northern California found as many as 45% of pediatric hospitalizations were found unlikely to have been caused by SARS-CoV-2. Similarly, 40% of patients under age 22 classified as “COVID” at another California hospital were incidental positives. Applying these percentages to the HHS data gives us .0086% of infections hospitalized because of COVID.
How does this compare to flu?
We don’t test for flu (or for any virus) like we do for SARS-CoV-2, including automatically upon hospital admission during flu season. But the CDC does maintain estimates. For example, the estimated rate for the 2017-2018 season was .128% for the 0-4 group and .038% for 5-17. Without question, flu carries a higher risk for hospitalization than COVID for younger kids. The risk for older kids and teens appears comparably lower than flu, but also depends on a child's or teen’s overall health.
One thing is for certain: Dr. Nemetski has zero functional knowledge of how the covid data is curated, and lacks the broad knowledge base of the available relevant subject matter. She does a great job of distilling the CDC’s propaganda into succinct bullet points though.
Even the CDC has refrained from declaring there to be a causal link (or any link at all) between MIS-C and covid. And they even offer the qualification that some kids got MIS-C but didn’t have covid (kind of like the equal prevalence of long covid in kids who had covid and kids who never had covid). From the CDC website:
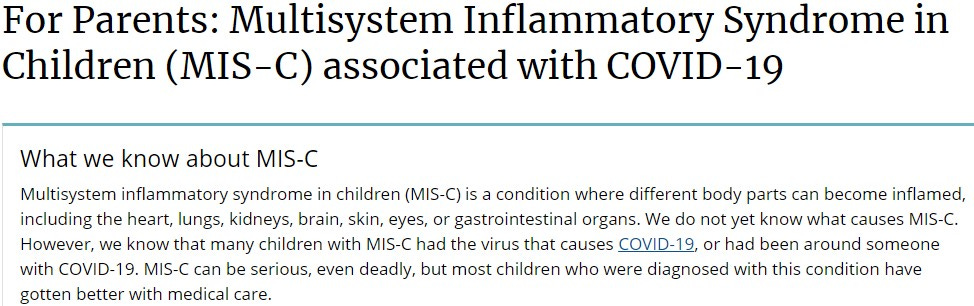
So apparently, Dr. Nemetzki can issue definitive statements where even the CDC itself acknowledges there exists a lack of clarity.
On the other hand, the Canadian study Environmental epidemiology of Kawasaki disease: Linking disease etiology, pathogenesis and global distribution found that Kawasaki (functionally renamed MIS-C last year)
“Patients with KD were generally less exposed to environmental allergens in many aspects of their daily lives (Table 3). They were more likely to primarily drink filtered or bottle water, were exposed less to household pets, were more likely to live in a dwelling constructed in the last 10 years and were less likely to live in an area with dense tree coverage, near a park, body of water or a farm. There was some statistically significant associations between the different exposures reported in Table 3.”
In other words, Kawasaki/MIS-C is more likely to occur in the absence of exposure to natural allergens and pathogens… a likely byproduct of lockdowns (which were of course strongly supported by JOWMA). Whoops.
Furthermore, there has not yet been any attempt as far as I’m aware of to quantify the epidemiological impacts of the covid policies on the health of the population, such as prolonged wearing of facemasks, lockdowns, social isolation, diet, exercise, and various markers of health, among other factors. Simply claiming that any adverse conditions found in anyone without a clear or observable cause is attributable to covid is rank negligence unbefitting a high school student, much less amply credentialed medical practitioners and health experts.
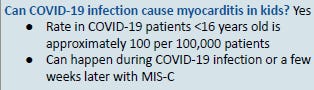
I’ll say this: if there was a 1/1000 myocarditis rate in kids with covid, you can bet there would’ve been hundreds of stories flying around the frum chats about it. This is fairy tale la-la land crackpot conjecture.
There has never been any sort of serous controlled study that showed anything remotely approaching the fanatical numbers alleged by Dr. Nemetzky. On the other hand, from hundreds of thousands of college covid cases, there were a handful of hospitalizations and *maybe* one death. No spate of myocarditis cases.
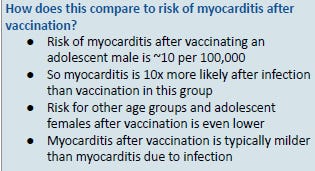
The major JAMA study on covid myocarditis in athletes admitted that 28 of the 37 myocarditis cases were “subclinical”, but this was compared to only clinical myocarditis cases from the vaccine to arrive at the conclusion that myocarditis was more prevalent from covid than from the vaccine.
The obvious truth of children’s lack of susceptibility to covid was even acknowledged in JAMA early on:
A 5/11/20 JAMA report 46 from U.S. and Canadian Pediatric Intensive Care Units (PICUs) confirmed the rarity of serious pediatric covid-19 disease noting: “most PICUs across North America reporting no children admitted with this disease during the study period”; despite the fact that “more than 80% [of the small number admitted] had significant long-term underlying medical conditions”…most commonly “long-term dependence on technological support associated with developmental delay and/or genetic anomalies…overall survival and outcomes from critical illness in infants and children with COVID-19 was far better than reported for adult patients.” The authors concluded, “our data indicate that children are at far greater risk of critical illness from influenza than from COVID-19.”
Nothing about myocarditis. (And this is hardly a one-off, for those who are thinking that this study didn’t take into account a longer window for observing myocarditis manifesting subsequent to covid, etc.)
From Pfizer's FDA briefing document:
Under Scenario 3 (lowest incidence), the model predicts more excess hospitalizations due to vaccine-related myocarditis/pericarditis compared to prevented hospitalizations due to COVID-19 in males and in both sexes combined."
Bear in mind, this is comparing *ONE* side effect of the vaccines against the totality of severe covid problems, and myocarditis is not even the most prevalent cause for post-vaccine hospitalization or death.
I guess Pfizer just felt like making insane contentions that have no basis in reality to malign their own product.
Perhaps, Dr. Nemetzky, you ought to read Pfizer’s own material for starters???
(Also, there is no way in a million years that Pfizer’s estimations are remotely accurate. They are definitely radically lowballing the myocarditis numbers. (See Part 2 for more on this.))
Onwards.
These changes resulted in an increase of the PULS score from 11% 5 yr ACS risk to 25% 5 yr ACS risk. At the time of this report, these changes persist for at least 2.5 months post second dose of a vaccine. We conclude that the mRNA vaccines dramatically increase inflammation on the endothelium and T cell infiltration of cardiac muscle and may account for the observations of increased thrombosis, cardiomyopathy, and other vascular events following vaccination.
Since December, 183 professional athletes, coaches and college and youth athletes have collapsed abruptly, and 108 have died. Some of the athletes, such as football stars Sergio Aguero and Christian Eriksen, collapsed in the middle of a game, in front of the spectators. The main cause: Cardiac problems - myo/pericarditis, cardiac arrest and heart attacks. What causes the sudden epidemic?
Mystery rise in heart attacks from blocked arteries | Scotland | The Times
Israeli Data Favor Higher Estimates of Post-Vax Myocarditis | MedPage Today
Puzzling heart diseases in football
From Daniel Horowitz:
A preprint from University of California Davis found that "for boys 12-15 without medical comorbidities receiving their second mRNA vaccination dose, the rate of CAE [cardiac adverse event ] is 3.7 to 6.1 times higher than their 120-day COVID-19 hospitalization risk as of August 21, 2021."
A recent study of the Danish population published in the Pediatric Infectious Disease Journal found that "the incidence of myopericarditis after COVID-19 vaccination among males appears higher than reports from the United States."
In September, the U.K. Telegraph reported, "Data from Public Health England (PHE) shows that during that period there were 2,103 extra death registrations with ischemic heart disease, 1,552 with heart failure, as well as an extra 760 deaths with cerebrovascular diseases such as stroke and aneurysm and 3,915 with other circulatory diseases."
But of course it’s not the vaccines.

You gotta love how absolutely definitive the propagandists are. Pretending as though this is even remotely “settled science” is mind-numbing chutzpah.
Long Covid in children is functionally almost nonexistent:
Prospective Study: Children and young people with Long Covid (CLoCK)
How Common Is Long COVID in Children and Adolescents? : The Pediatric Infectious Disease Journal
The upshot is that long covid in children is so exceedingly rare as to be a largely mythical condition.
Anyway, here is more from Emily Burns to put the final nail into the Long Covid coffin:
What about the risk of so-called “long COVID”?
In general, as researchers from the U.K. put it, COVID is short-duration and of low symptom burden in school-aged children. Viral infections of many kinds can have lingering symptoms. (See thread by @heckofaliberal for examples.) Some could be described as “severe”, others merely annoying. But SARS-CoV-2 does not yet appear to be unique, higher prevalence, or greater severity for children in this regard.
Findings from several studies follow:
A study of ~1,700 symptomatic children in the U.K. who tested positive for SARS-CoV-2 showed very low rates of prolonged symptoms at 4 weeks post-illness:(4.4%) and <2% beyond 2 months. Severity symptoms was worse in 15 kids in a control group who were not diagnosed with COVID.
Another study of 171 Australian children found 95% had very mild or asymptomatic illness, and low rates of mild symptoms at 3-6 month follow-up. By the end of the study, all children were back to baseline health.
Swiss researchers found no difference between seropositive and seronegative children with symptoms beyond 4 weeks (~10%), and similarly very low rates of symptoms at 6 months (2% and 4%). The most common long-term symptoms were fatigue, headache, & loss of smell.
In Germany, 35% of 1,500+ teens in one study (~1,300 of whom were seronegative for SARS-CoV-2 and ~200 seropositive) reported symptoms associated with long COVID, such as difficulty concentrating, headache, abdominal pain, fatigue, insomnia, and sadness. However, there was no statistical difference between the two groups of students, prompting the researchers to raise the question of whether “Long-COVID19” is really “Long-Pandemic Syndrome”.
Unless new data suggest otherwise, both the very low rate of persistent symptoms - and the low “grade” and duration of those symptoms - further support my claim that COVID illness doesn’t lead to severe outcomes for all but the fewest children.
Children are not threatened by covid, and certainly do not need a vaccine whose safety is a mess, whose efficacy is negative after six months, and was never needed at all because there are numerous highly effective prophylactic and treatment options that work better then and without the safety issues of these vaccines.
There is demonstrably no need to worry about kids. There is certainly no upside to making a big machlokes in the community about vaccinating children. Is it really too much to ask that the medical community at least leave the kids alone??
Debunking JOWMA's Latest Brazenly False Ad About Covid and Children, Part 2